Downloaded 298 times

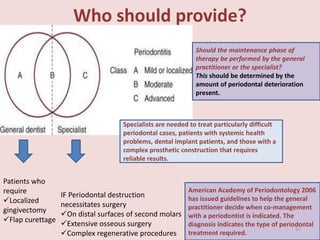
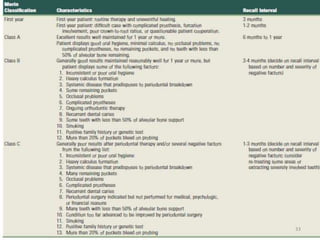
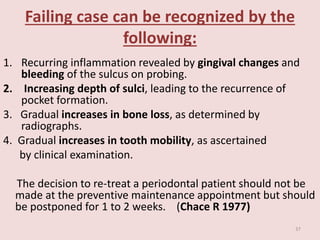


Supportive periodontal therapy (SPT) involves long-term maintenance programs following active periodontal treatment to maintain periodontal health. SPT involves periodic examination, motivation and instrumentation of sites showing inflammation, treatment of reinfected sites, and polishing. It begins after active treatment and is aimed at preventing recurrence through early detection of disease. The frequency of SPT visits depends on the patient's periodontal risk assessment but generally occurs every 3-4 months. It can be performed by general dentists or specialists depending on the extent of original periodontal destruction. Adjunctive use of antimicrobials may also be included in SPT.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








