Download as PDF, PPTX
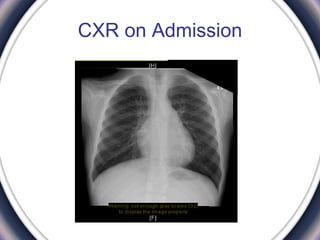
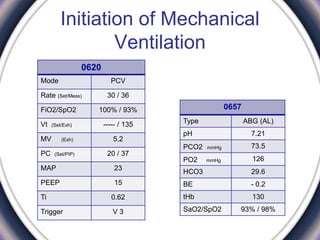
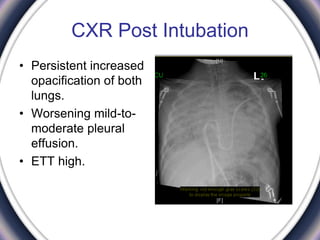
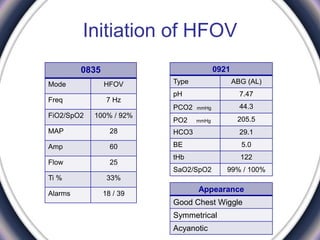
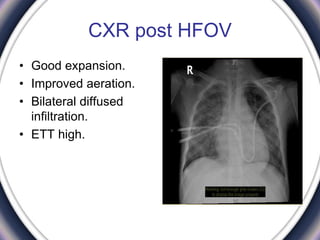
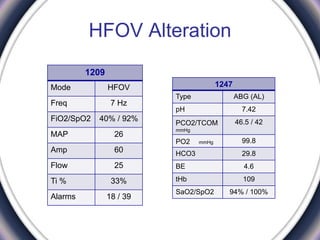
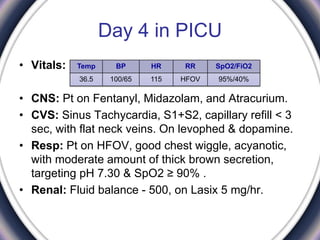
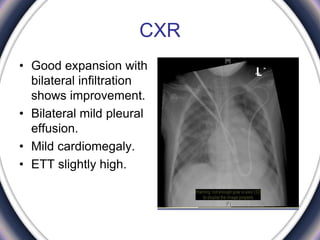
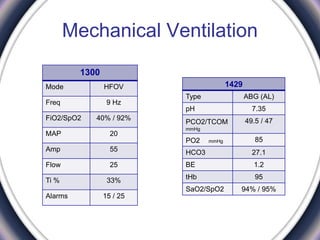
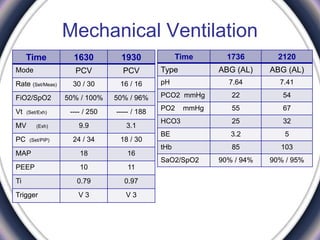
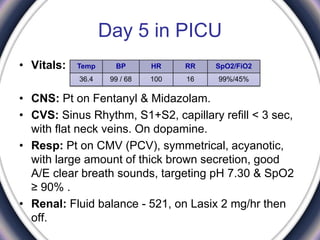
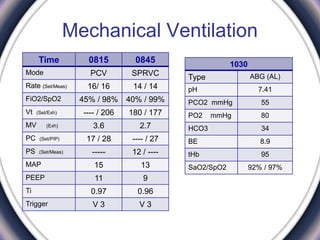
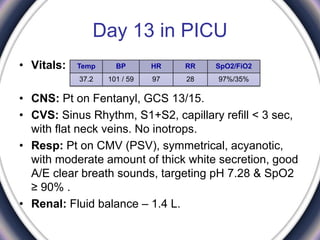
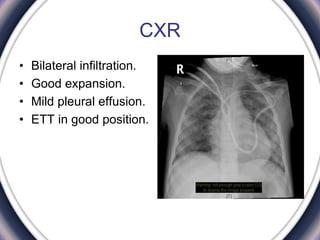
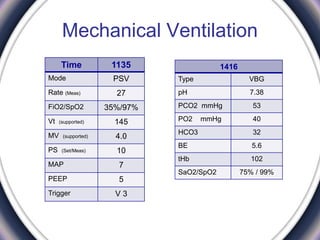
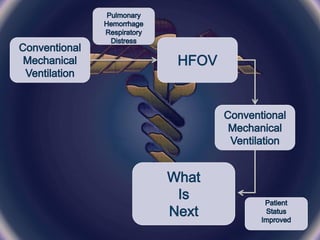
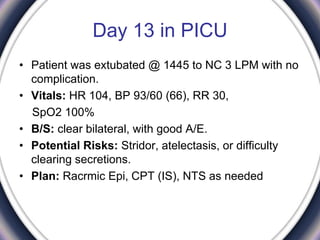
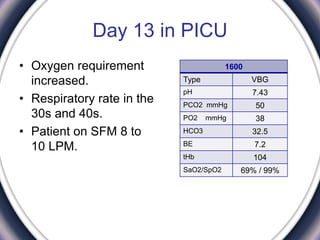
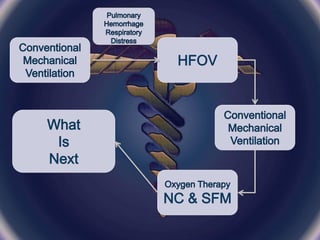
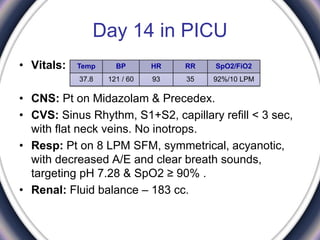
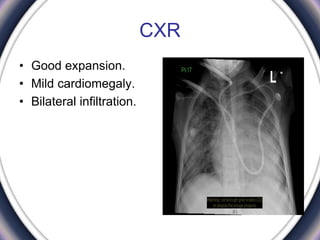
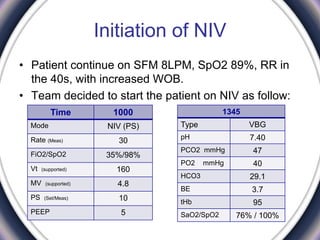
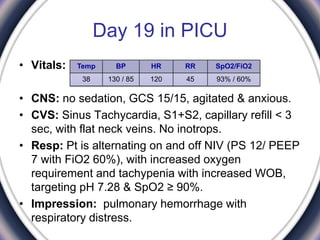
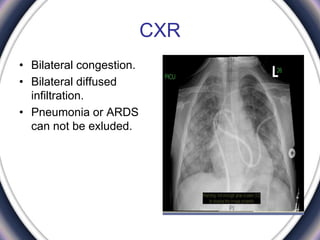
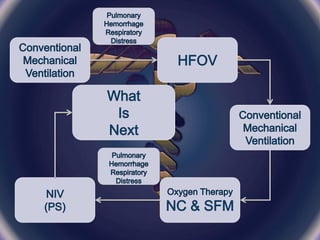
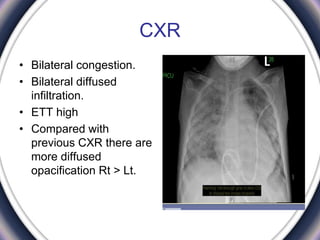
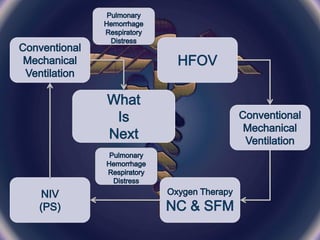
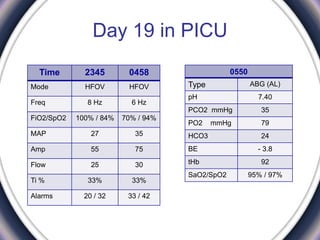
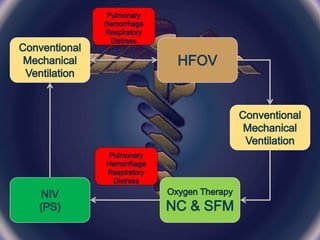


- A 9-year-old girl with beta thalassemia major was admitted to the PICU for respiratory distress following an allogenic stem cell transplant. She required intubation and mechanical ventilation support. - Various ventilation modes were trialed, including PCV, HFOV, PSV and NIV. Weaning attempts were made but oxygen requirements increased, requiring reintubation. Bilateral infiltrates were seen on chest x-rays. - After 19 days in the PICU receiving respiratory support and undergoing further weaning trials on various modes, the patient's condition remained critical with ongoing respiratory distress and oxygen needs.


































































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)



