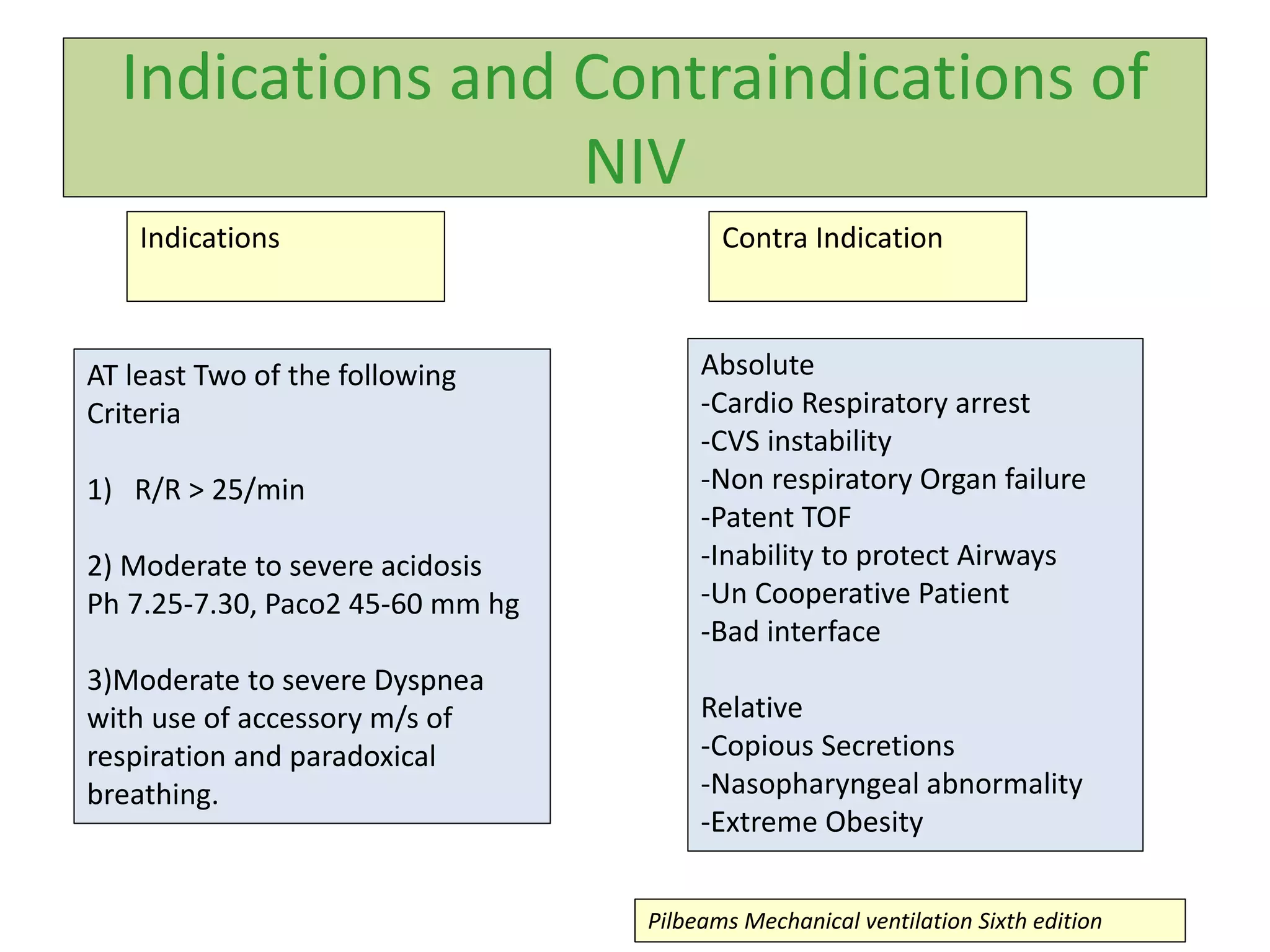
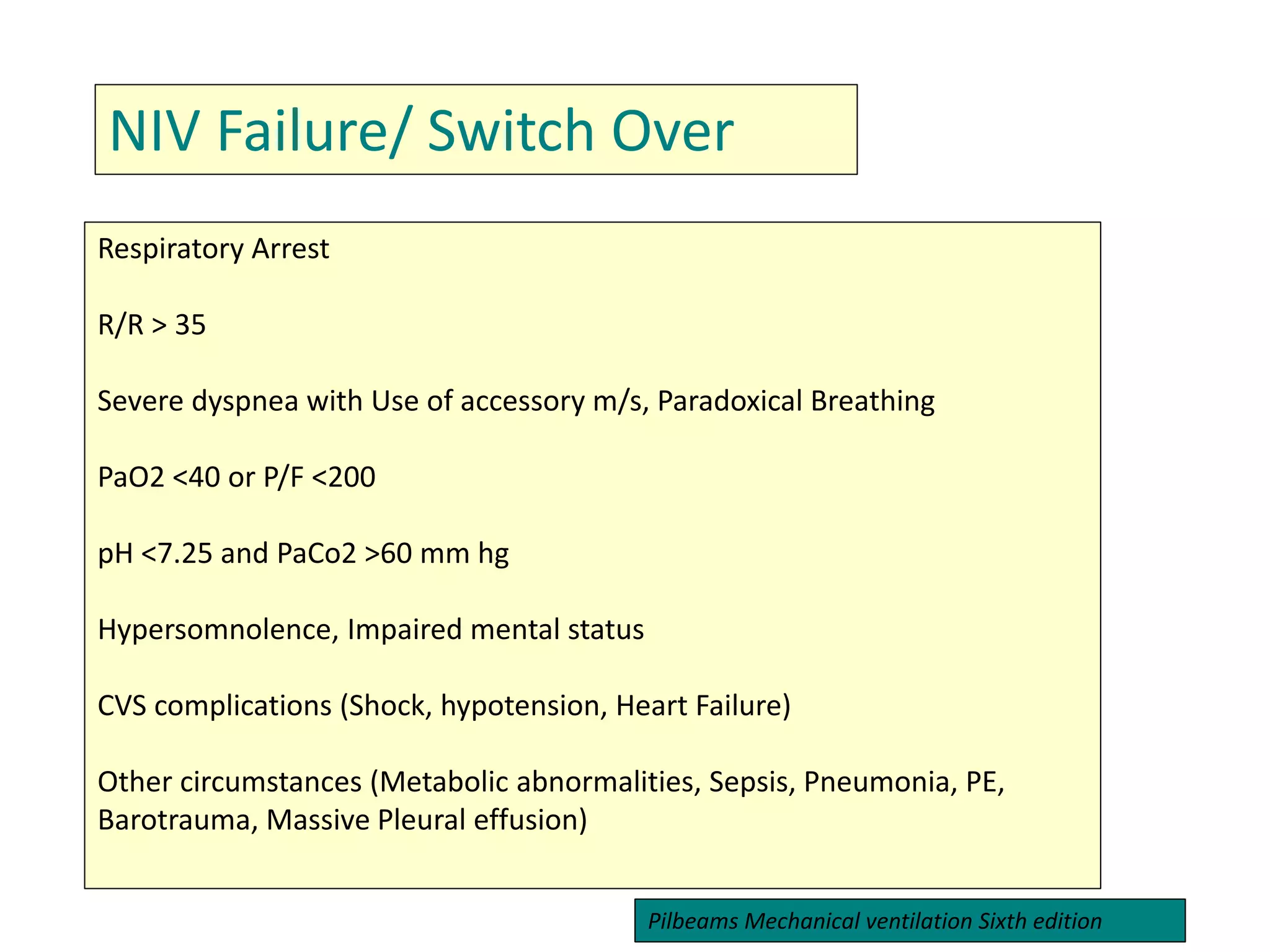
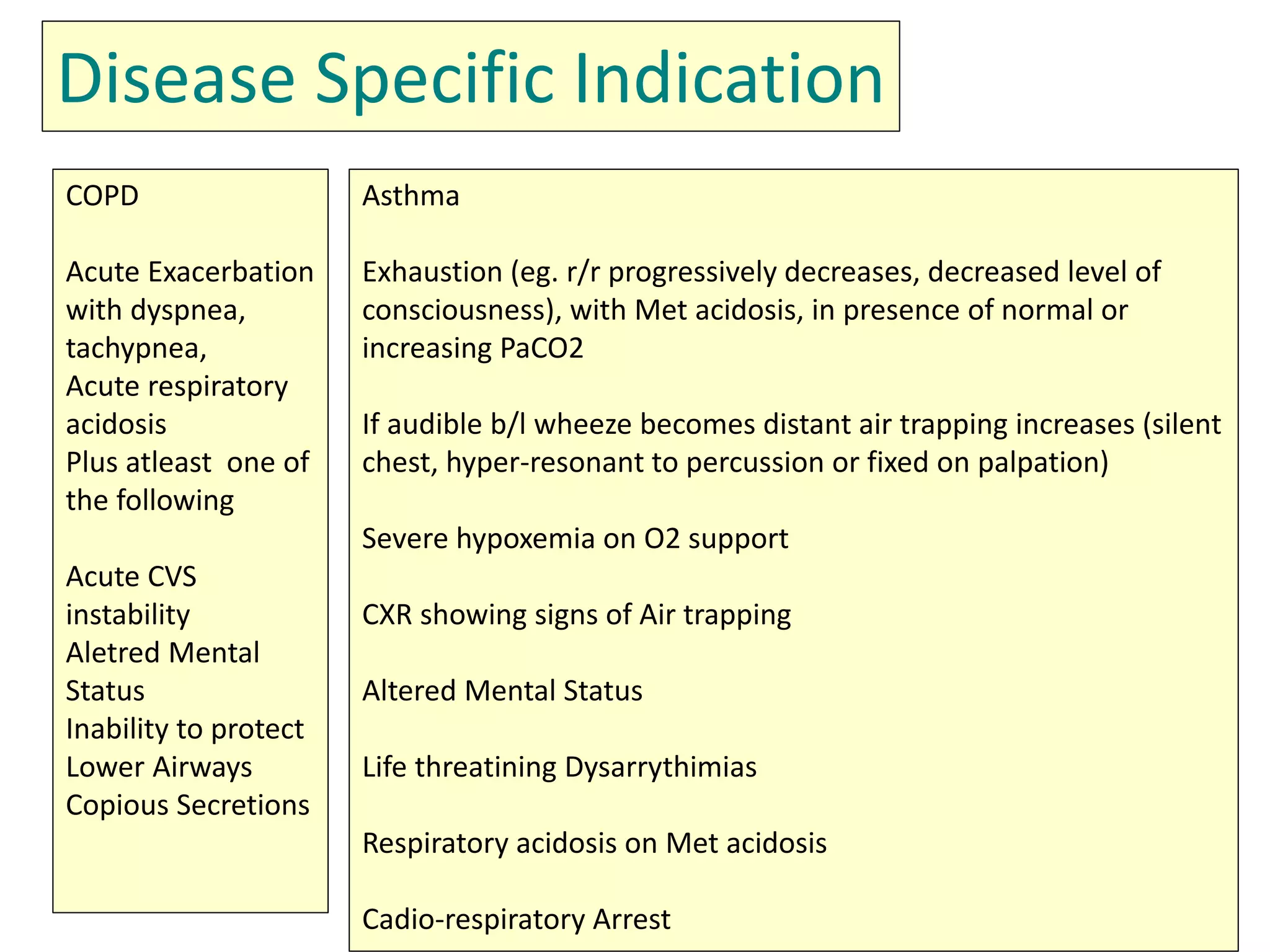
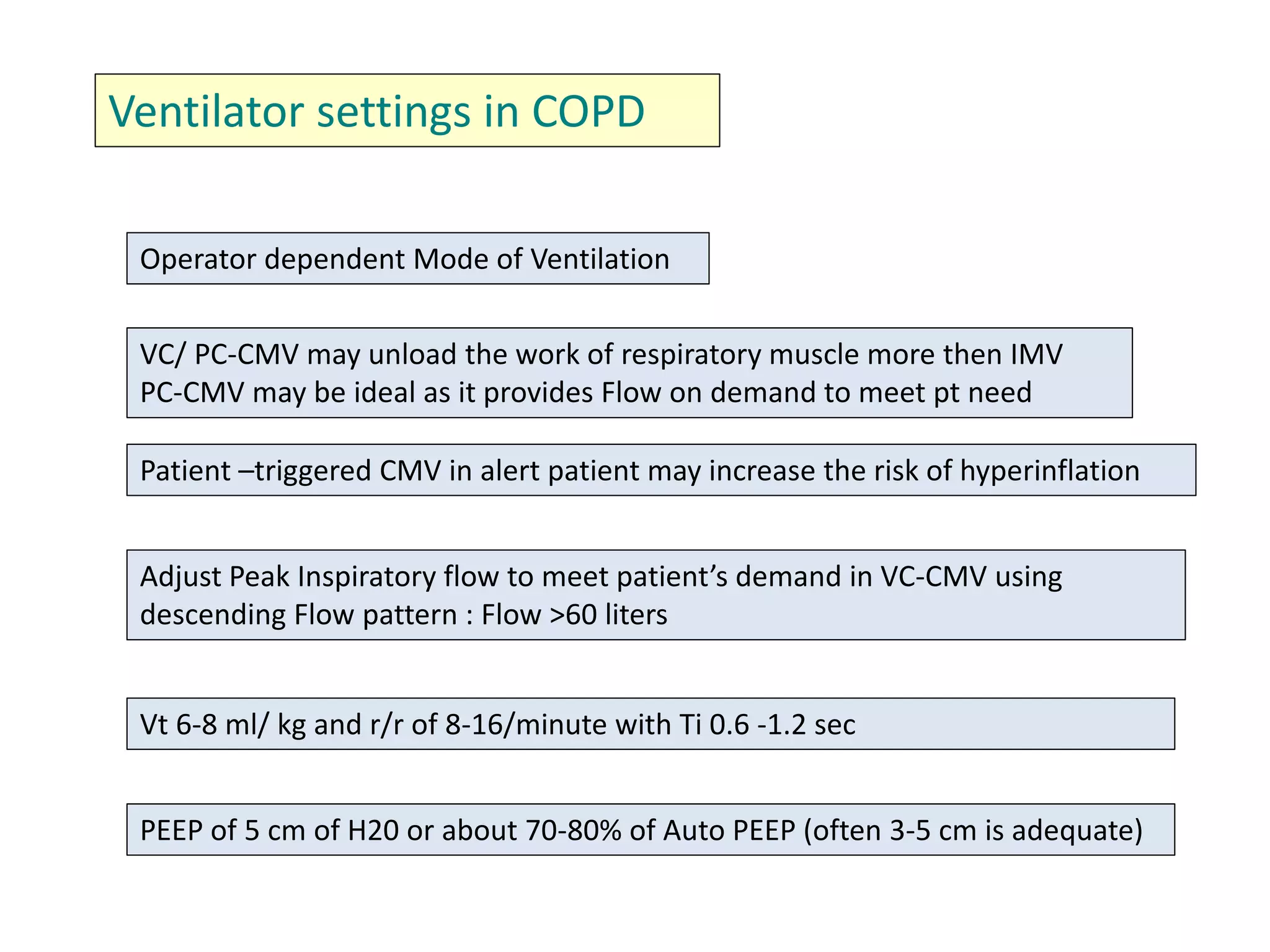
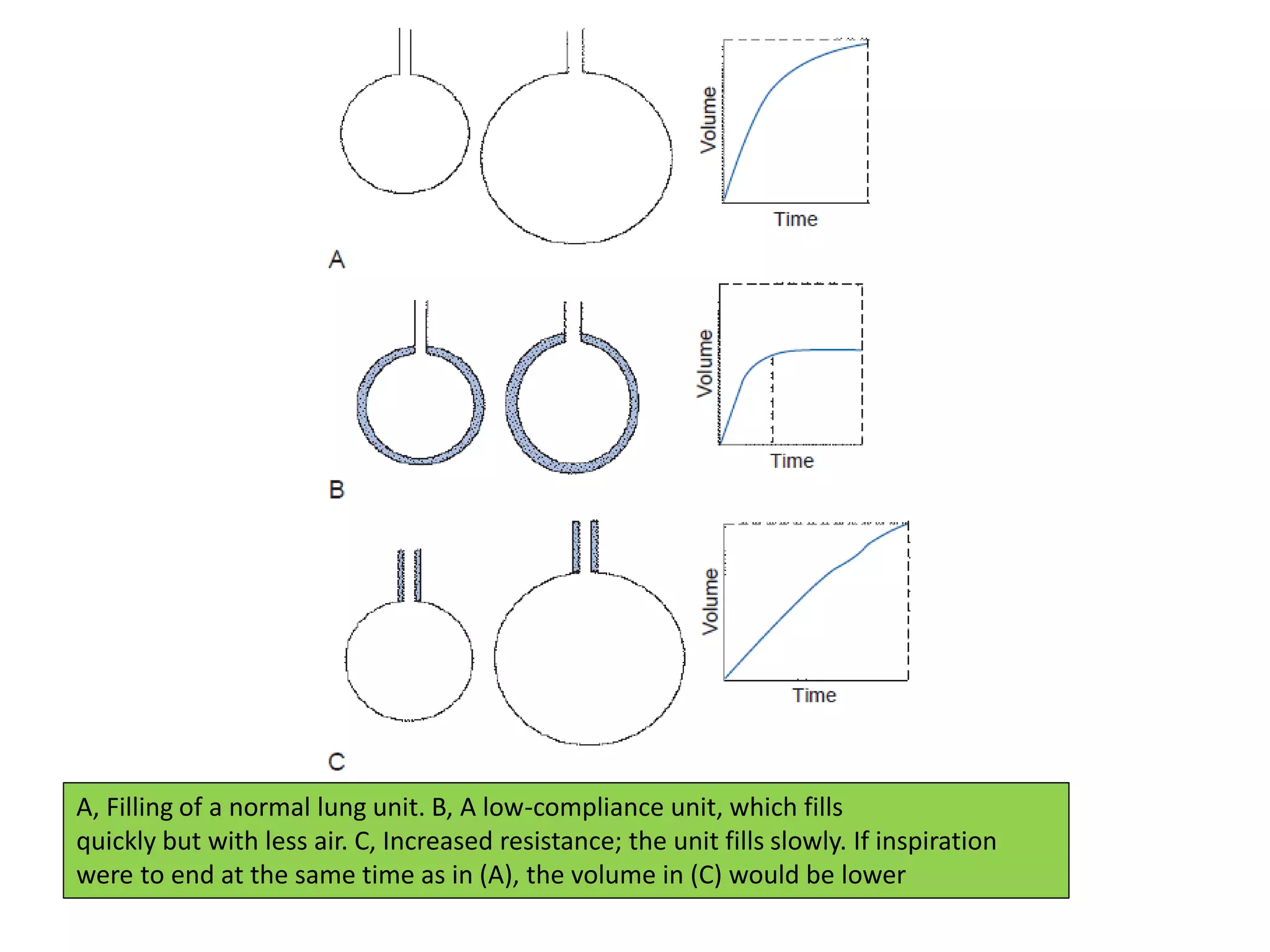
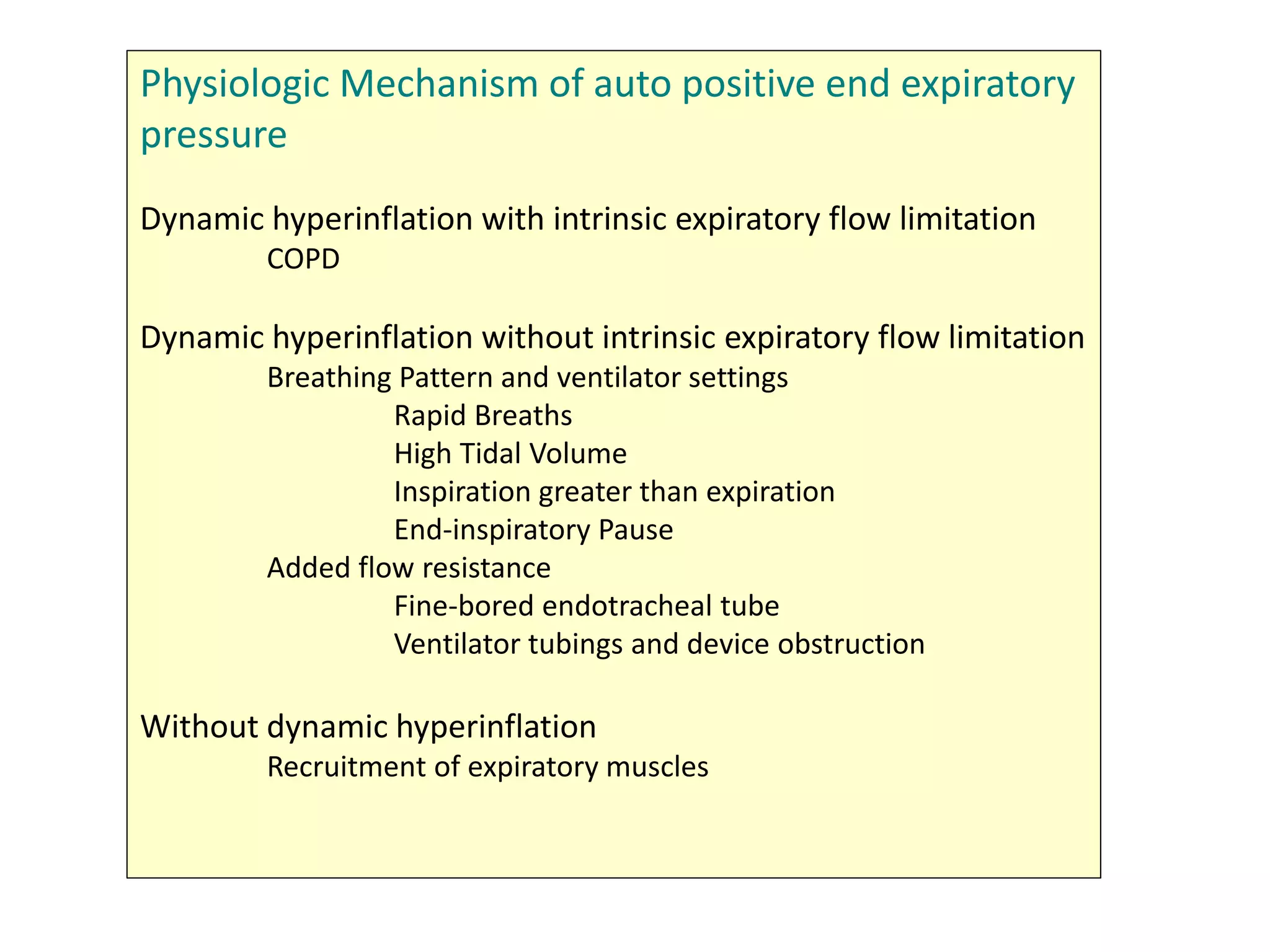
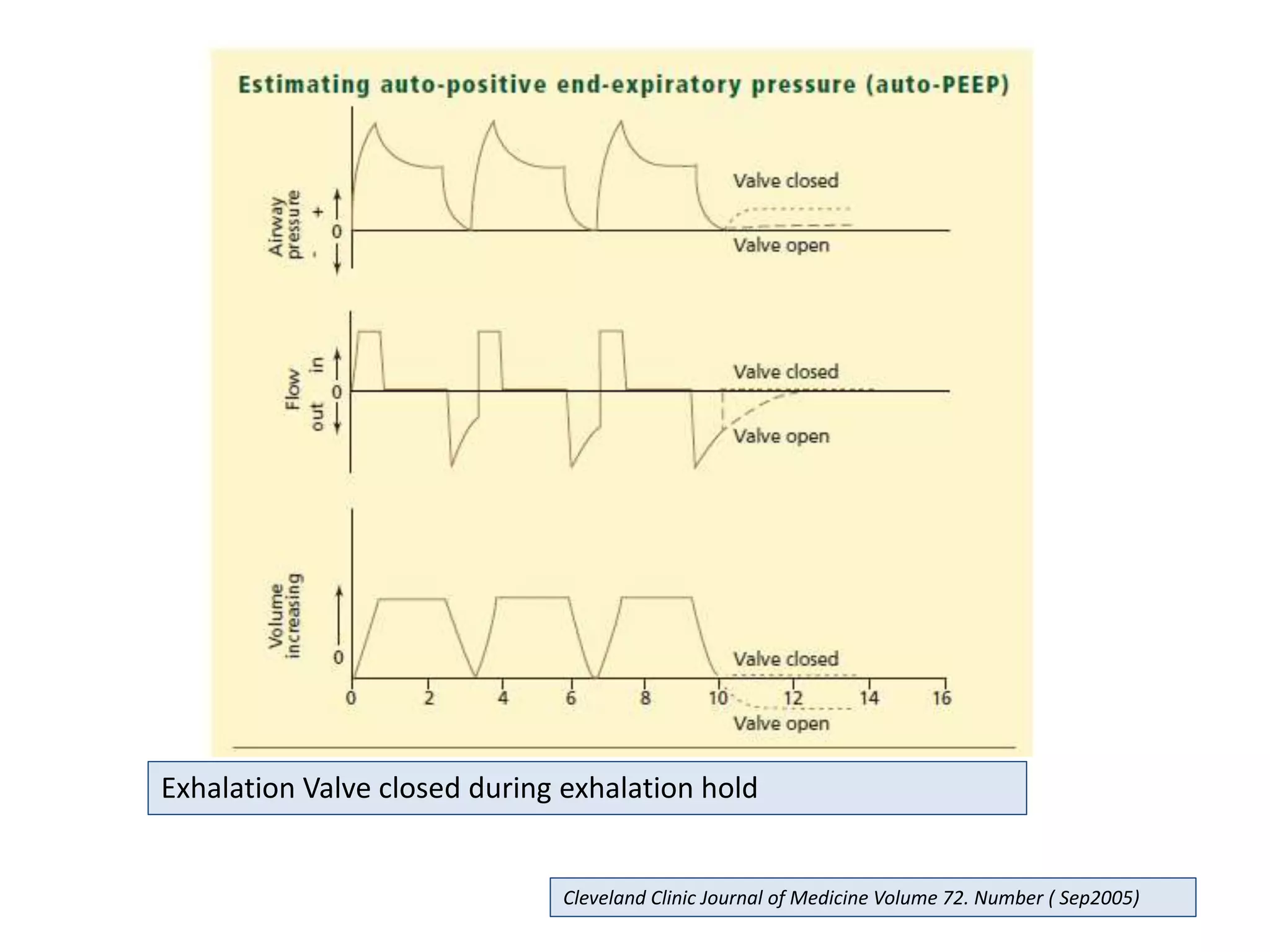
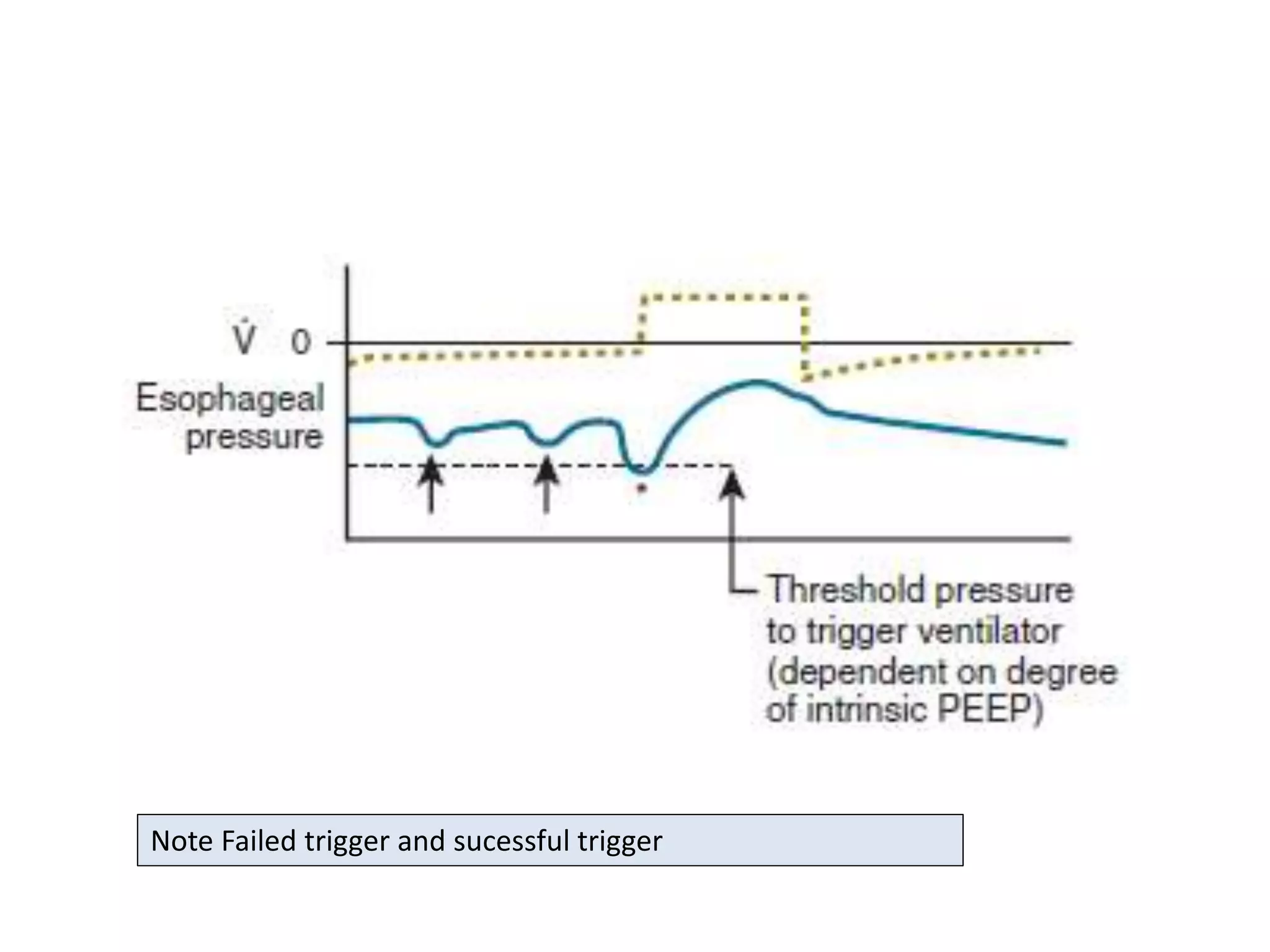
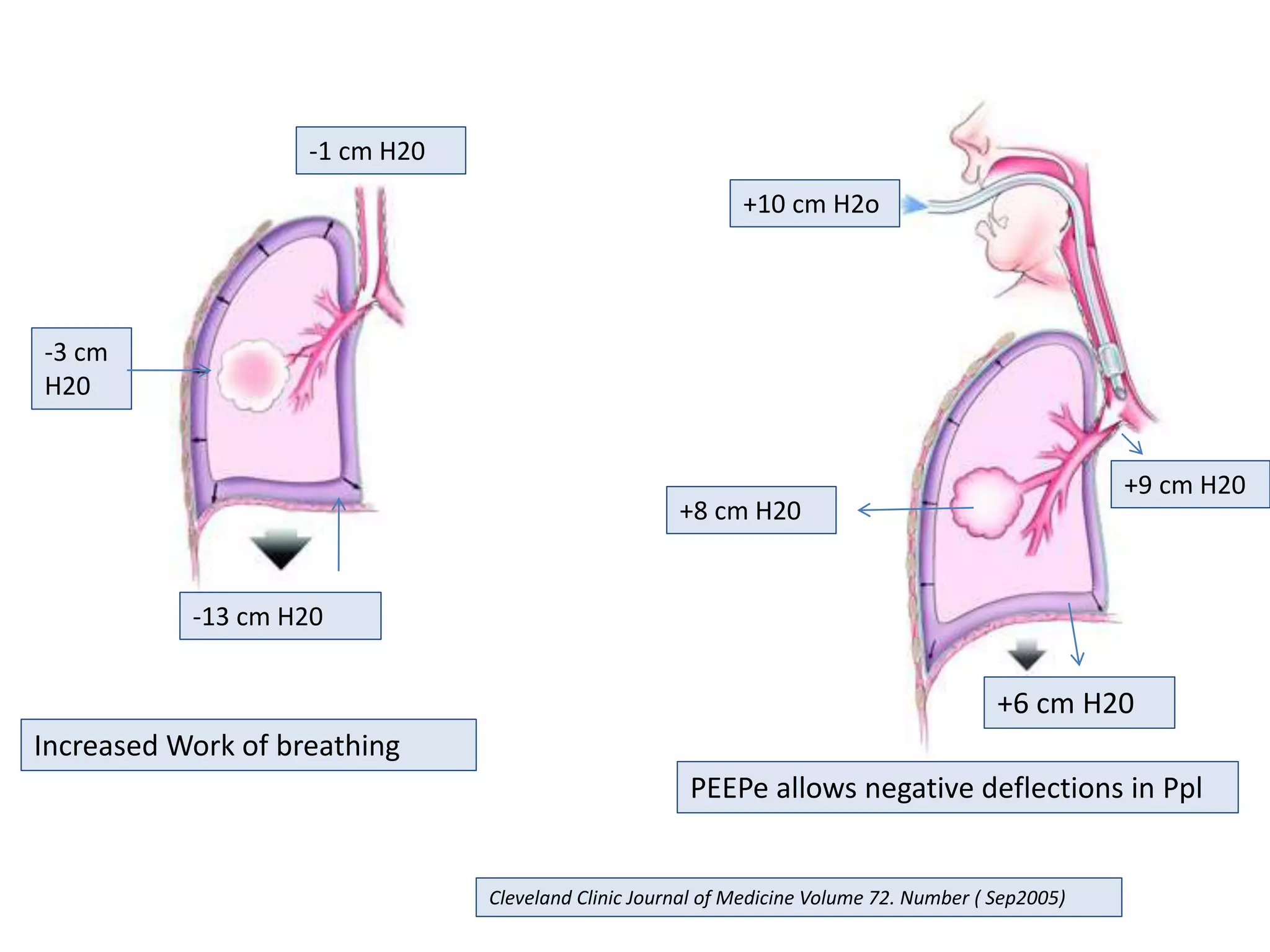
This document discusses ventilation in obstructive airway diseases. It provides indications and contraindications for non-invasive ventilation (NIV) including criteria such as respiratory rate greater than 25 breaths per minute and moderate to severe respiratory acidosis. NIV can be used to support patients with acute exacerbations of COPD or asthma to reverse respiratory failure. Ventilator settings aim to support gas exchange, reduce work of breathing, and prevent complications. Dynamic hyperinflation can cause auto-PEEP which increases workload and impairs hemodynamics. Settings to treat auto-PEEP include increasing expiratory time, reducing tidal volume, and applying external PEEP.






















![Mechanical ventilation[1]](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalventilation1-150109002450-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































