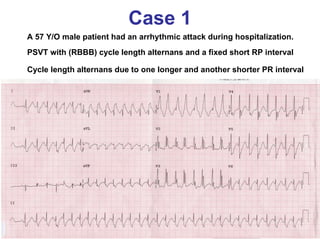
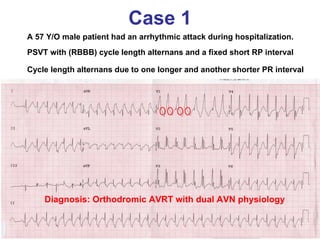
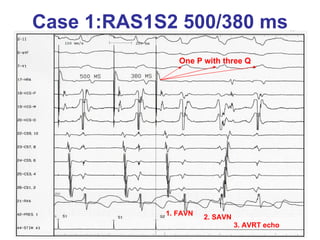
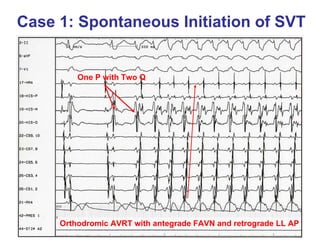
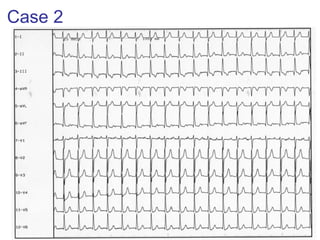
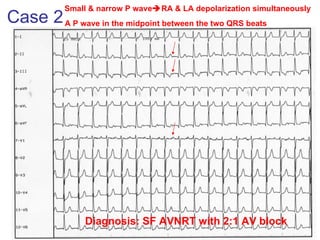
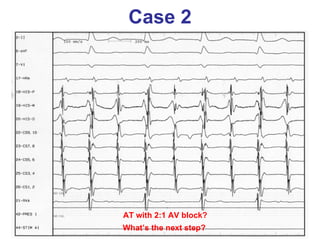
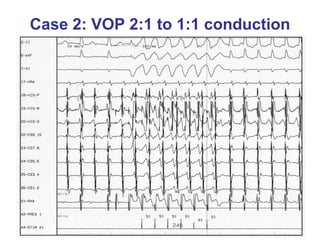

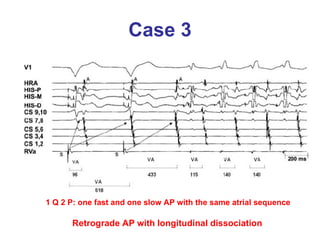
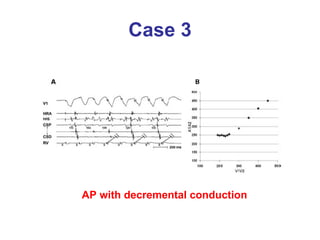

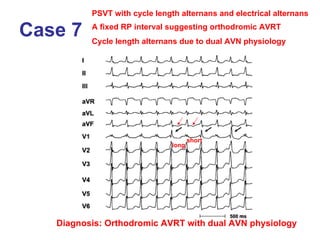

The document describes 10 cases of arrhythmias with electrocardiogram (ECG) findings. Case 1 involves paroxysmal supraventricular tachycardia (PSVT) with right bundle branch block (RBBB) and cycle length alternans due to dual atrioventricular node (AVN) physiology, consistent with orthodromic atrioventricular reentrant tachycardia (AVRT). Case 2 involves a narrow P wave indicating simultaneous right and left atrial depolarization, consistent with slow-fast AVNRT with 2:1 atrioventricular block. Case 3 demonstrates initiation of supraventricular tachycardia from normal sinus rhythm with preexcitation due to a retrograde