Download as PDF, PPTX
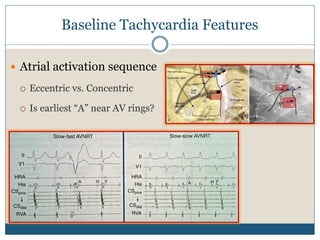
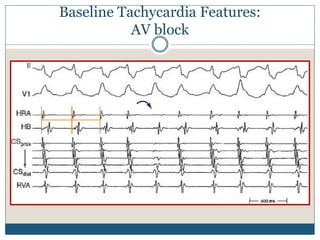
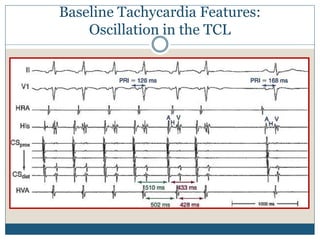
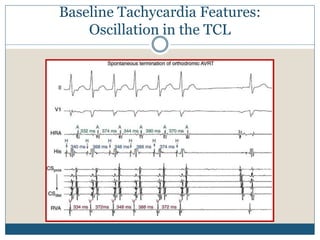
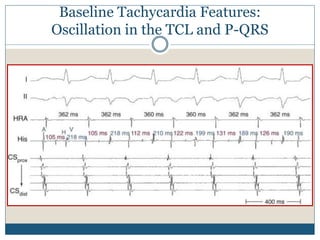
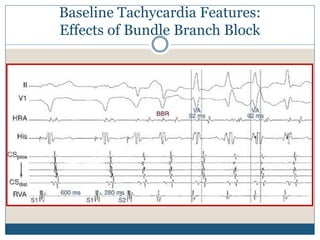
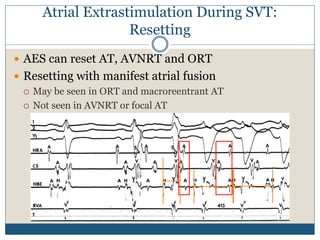
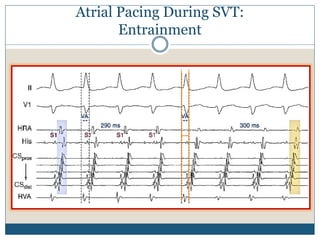
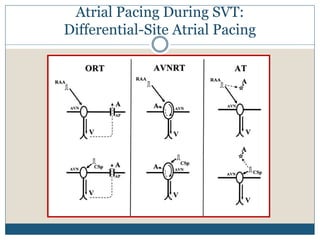
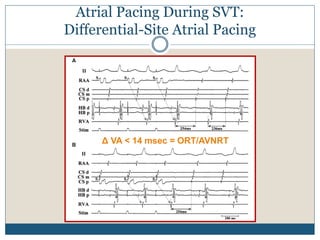
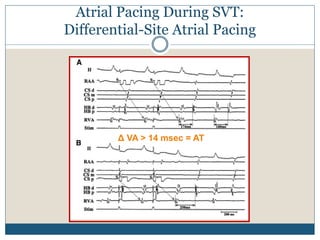
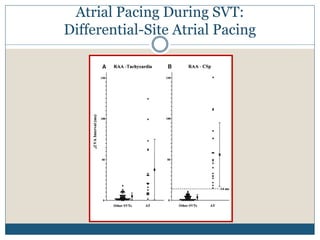
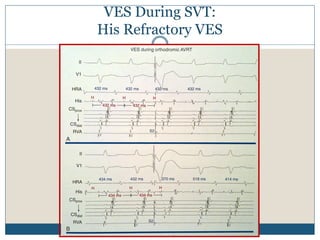
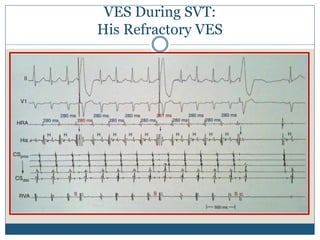
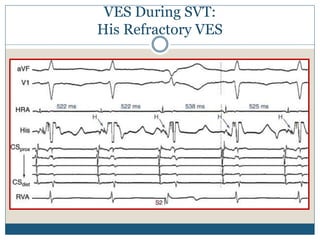
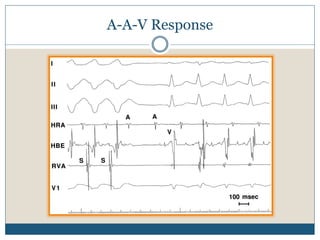
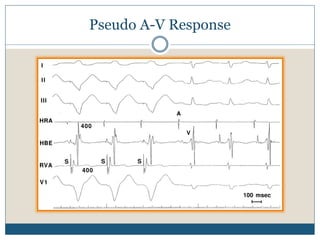

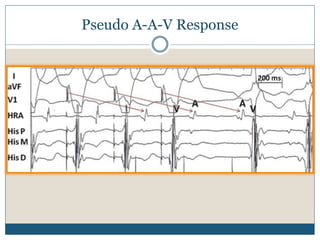
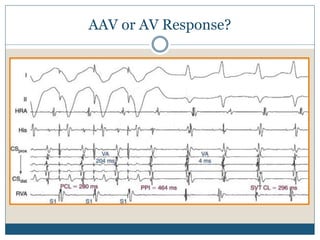
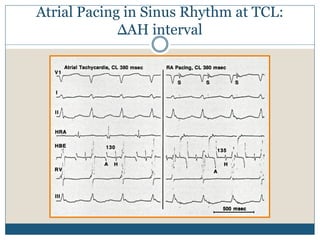
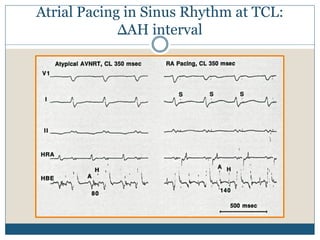
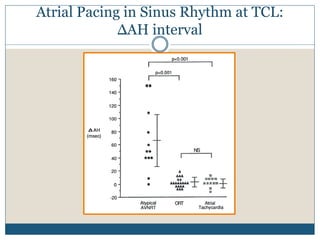
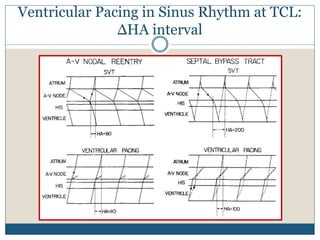
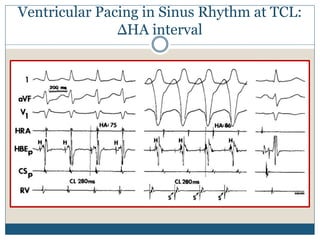
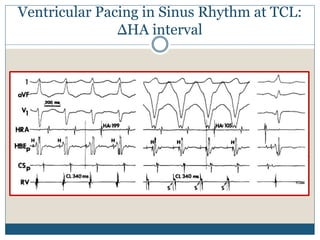
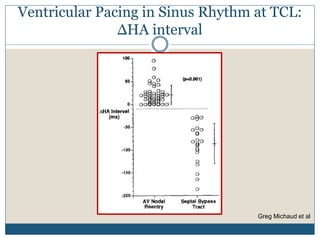

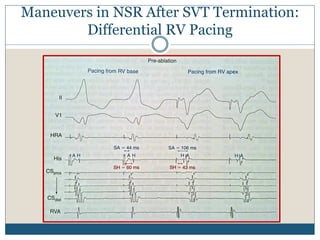
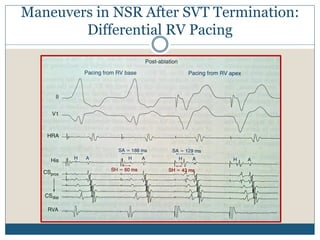
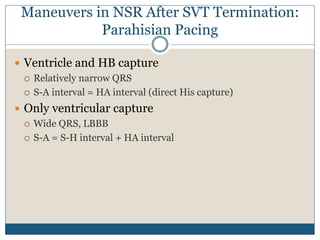
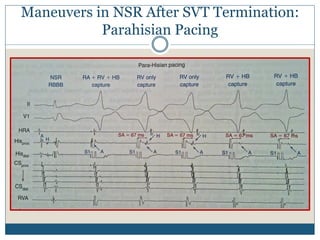
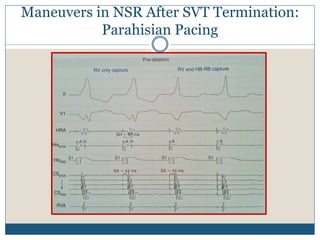
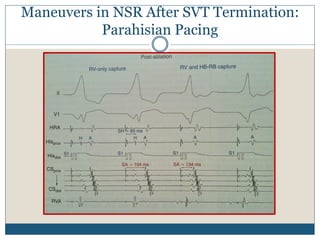
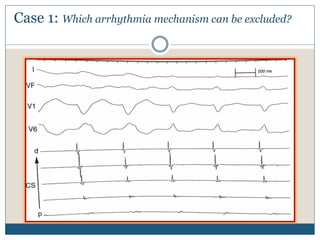
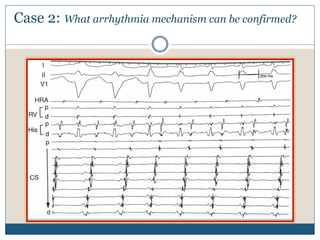
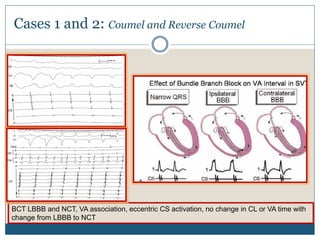
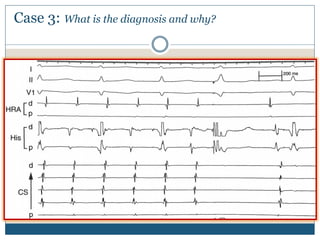
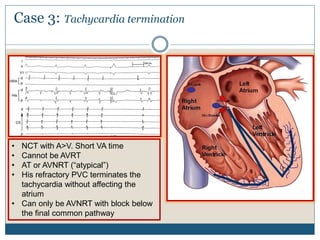
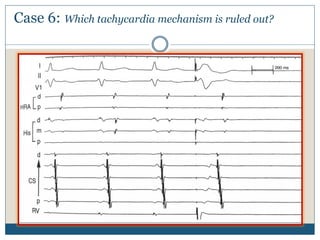
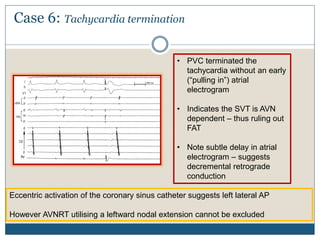
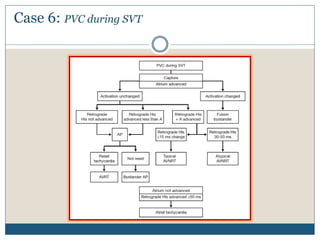
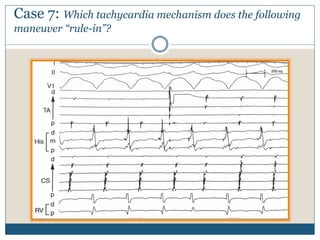

This document outlines techniques for differentiating supraventricular tachycardias (SVTs). It discusses features of SVT induction and baseline tachycardia characteristics, as well as diagnostic maneuvers that can be performed during tachycardia and after termination in sinus rhythm. These include the effects of atrial and ventricular extrastimulation or pacing on SVT cycle length, VA intervals, and atrial activation sequences to help identify the mechanism as atrial tachycardia, atrioventricular nodal reentrant tachycardia, or orthodromic reentrant tachycardia using an accessory atrioventricular connection. The document provides detailed descriptions and examples of applying these diagnostic tests.