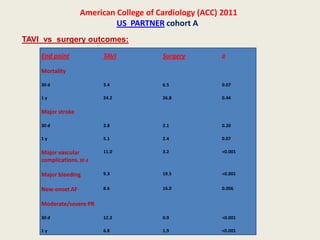
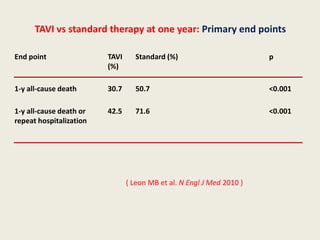
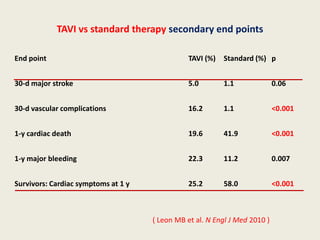
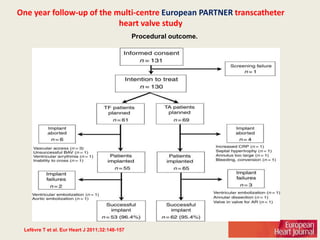
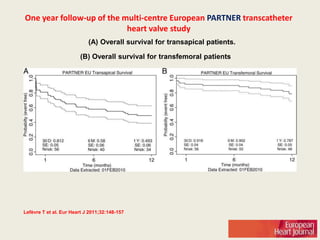
The document discusses transcatheter aortic valve implantation (TAVI), including its approval and increasing use in Europe and the United States. It provides details on the team approach, devices, procedures, outcomes, and complications of TAVI based on clinical trials such as PARTNER. TAVI is an alternative to surgical aortic valve replacement for high-risk or inoperable patients with severe aortic stenosis.