Downloaded 309 times



![• The extent of revascularization was
characterized by the British Cardiovascular
Intervention Society jeopardy score and
anatomical revascularization index, which was
calculated as follows: [(the pre-PCI jeopardy
score minus the post-PCI jeopardy score)
divided by (the pre-PCI jeopardy score)]×100,
with 100% indicating complete
revascularization of all angiographically
significant coronary disease](https://image.slidesharecdn.com/percutaneousrevascularizationforischemicleftventriculardysfunctionrevivedbcis2-220827134247-b51f126b/85/Percutaneous-Revascularization-for-Ischemic-Left-Ventricular-Dysfunction-REVIVED-BCIS-2-pptx-9-320.jpg)
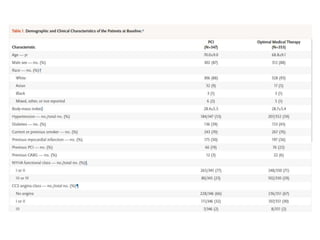
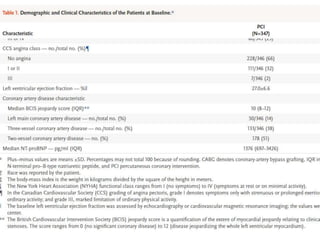

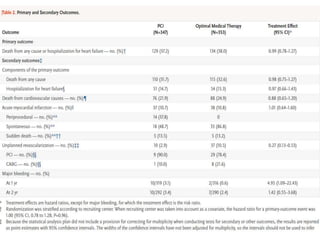
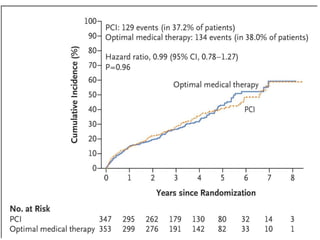
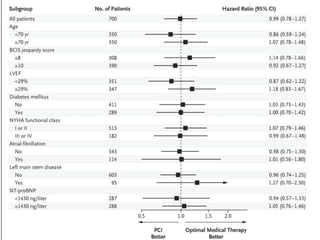
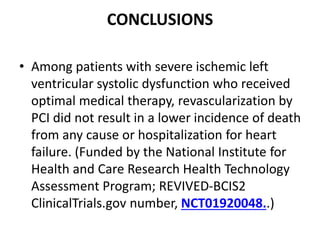

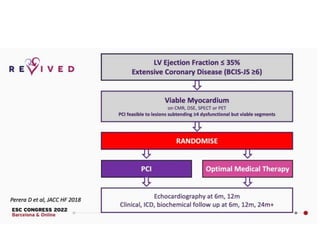
This study compared percutaneous coronary intervention (PCI) plus optimal medical therapy to optimal medical therapy alone in patients with severe left ventricular systolic dysfunction. Patients were randomly assigned to receive either PCI plus medical therapy or medical therapy alone. The primary outcome was death from any cause or hospitalization for heart failure. At 12 months, PCI did not result in a lower rate of the primary outcome compared to medical therapy alone. Extensive medical therapy was optimized for heart failure in both groups.
































![Revascularisation of non culprit lesion in acute mi [Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/revascularisationofnonculpritlesioninacutemiautosaved-1-260208144735-49d2f40b-thumbnail.jpg?width=640&height=640&fit=bounds)






















































