Download as PDF, PPTX
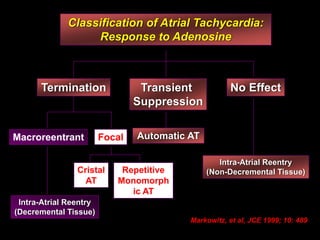
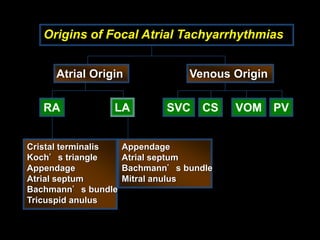
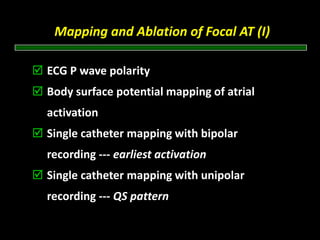
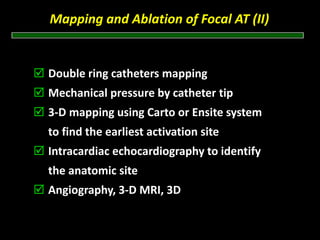
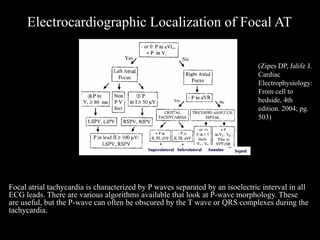
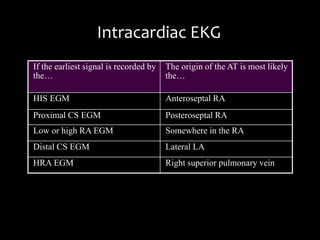
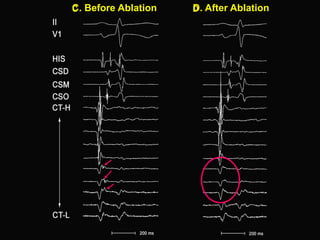
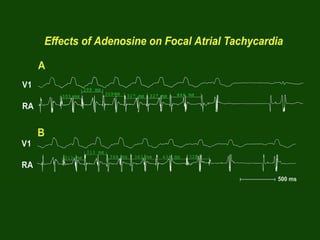
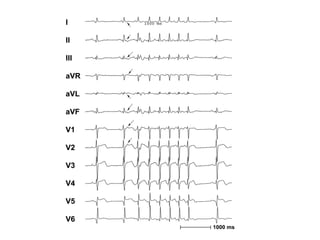
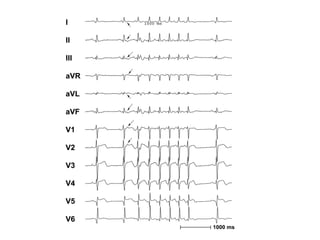
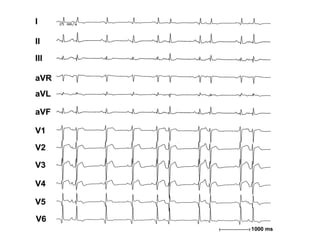
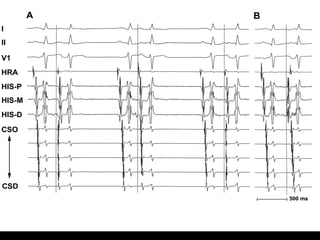
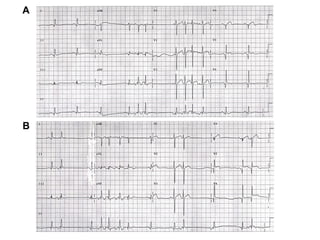
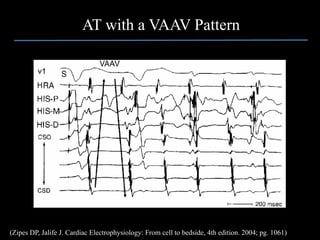

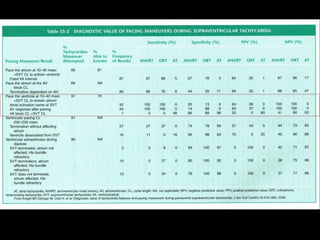
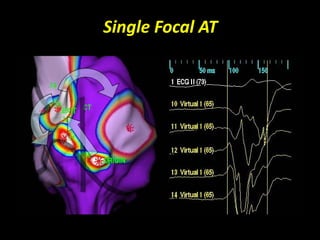

Atrial tachycardias are an uncommon cause of supraventricular tachycardia, accounting for around 5-15% of cases depending on whether the patient has congenital heart defects. Atrial tachycardias can be focal, originating from a single site, or macroreentrant utilizing existing anatomical barriers; 3D mapping systems have improved localization of focal atrial tachycardia origins by providing better atrial anatomy visualization. Successful focal atrial tachycardia ablation is identified by termination of tachycardia within 10 seconds of beginning radiofrequency delivery and inability to reinduce tachycardia with drug provocation.





























































![ECG [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/ecgcompatibilitymode-230828072404-d338c45c-thumbnail.jpg?width=640&height=640&fit=bounds)


























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















