
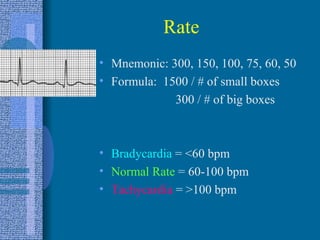
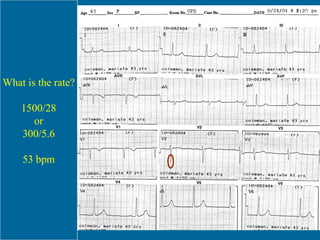
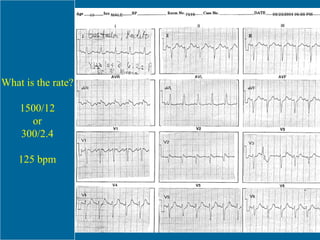
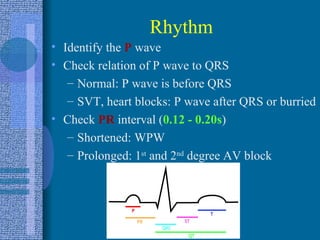
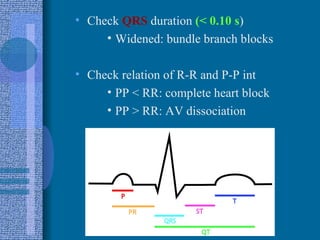

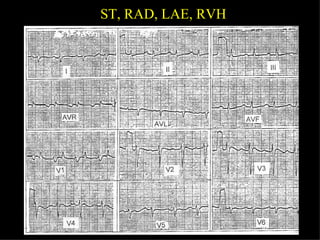

1. The document discusses electrocardiographic (ECG) interpretation including determining cardiac rate and rhythm, identifying conduction disturbances, myocardial ischemia or infarction, and other abnormalities. 2. It provides details on properly placing ECG leads and determining the cardiac axis. Common rhythms, conduction blocks, hypertrophy, and other ECG findings are explained. 3. A mnemonic device, RRAHIM, is presented to guide the systematic interpretation of an ECG, covering rate, rhythm, axis, hypertrophy, ischemia/infarction, and other findings.











































































































