Download as PDF, PPTX
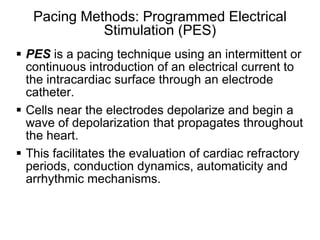
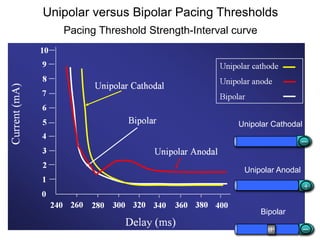
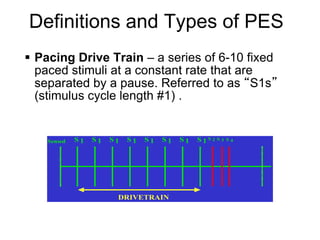
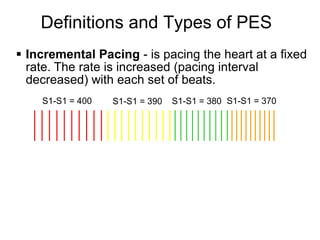
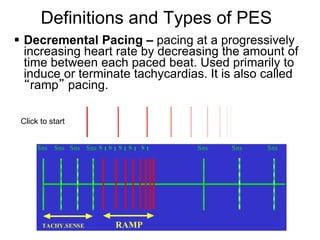
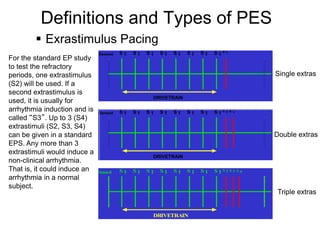
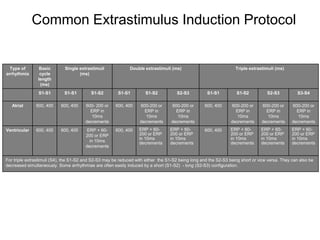
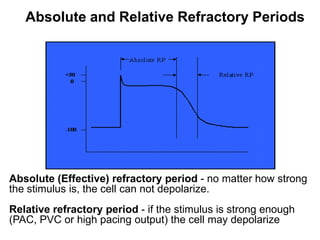
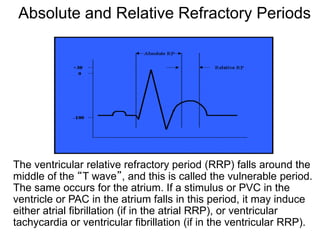
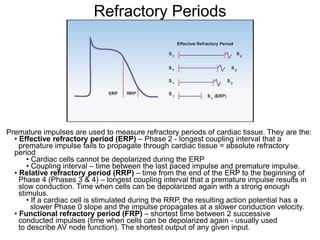
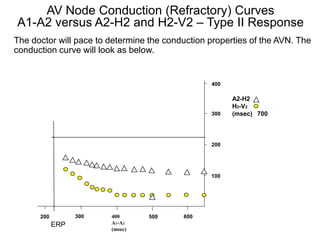
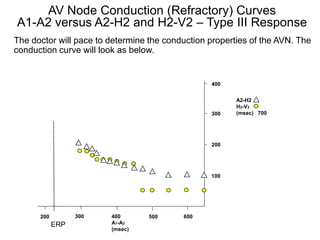
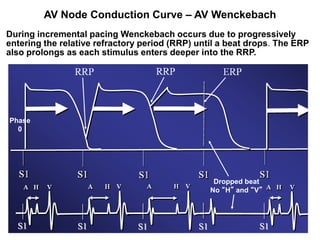
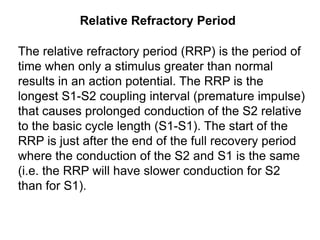
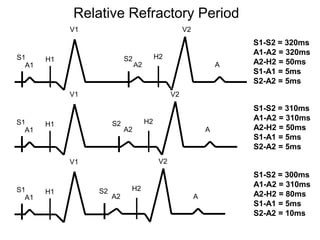
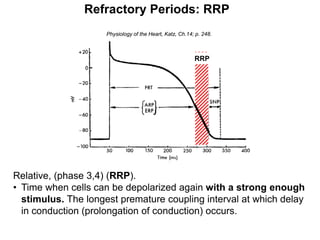
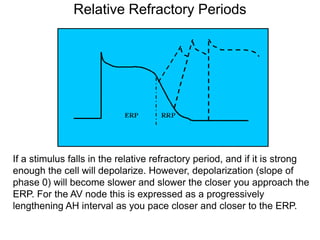
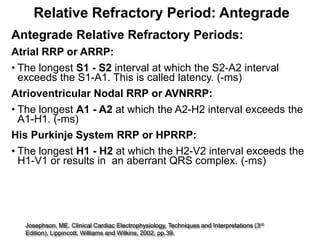
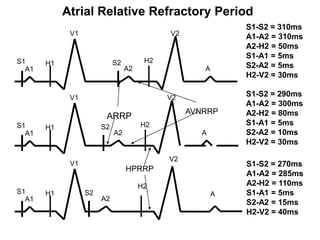
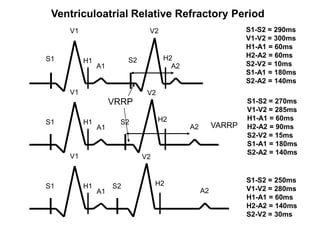
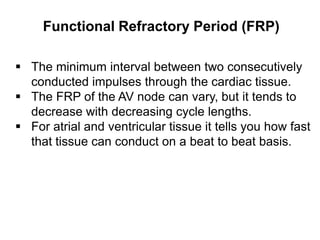
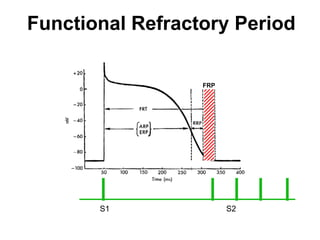
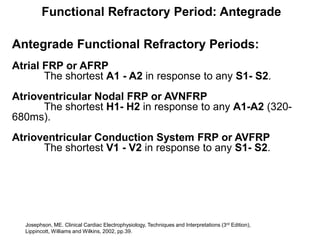
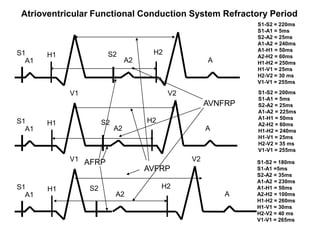
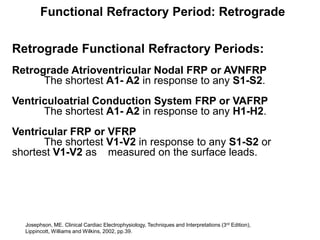
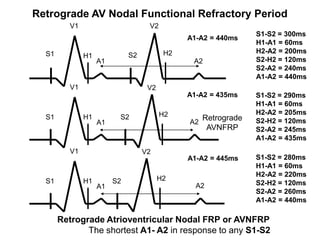
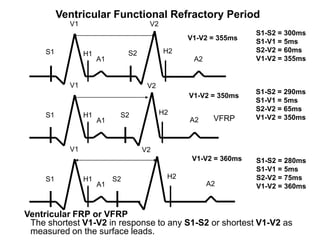
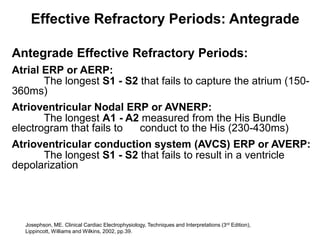
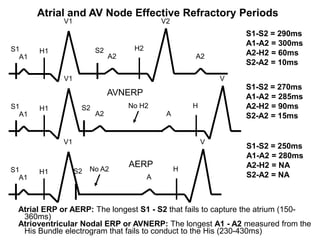
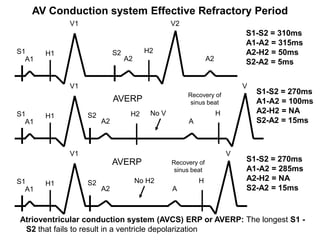
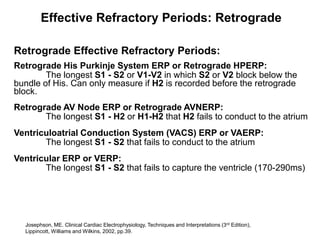
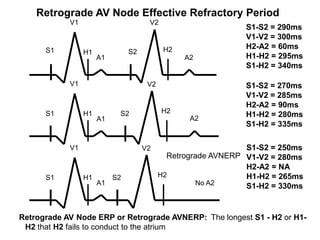
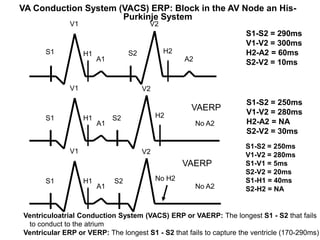
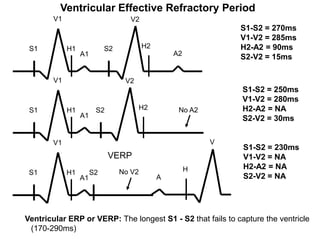
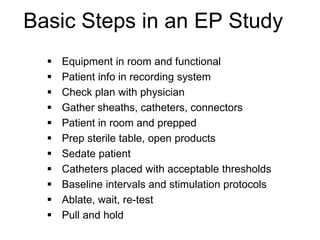

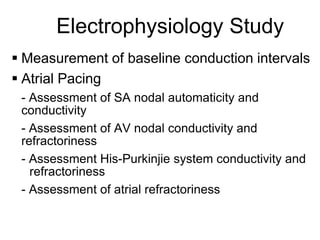
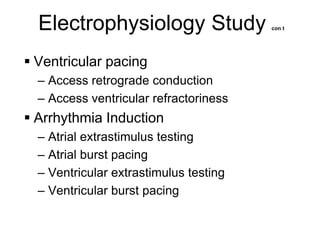
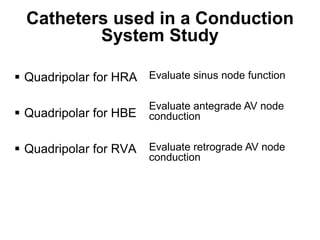
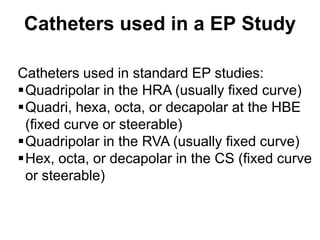
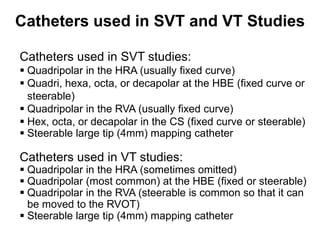
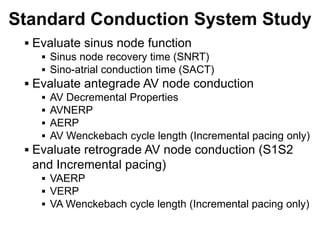
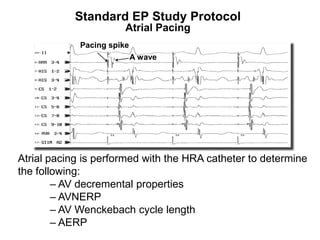
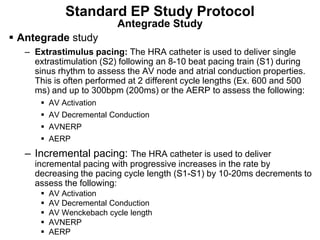
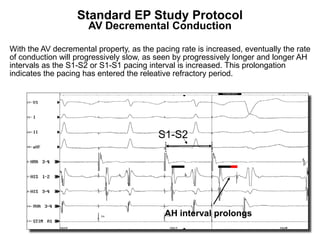
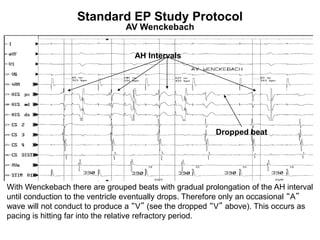
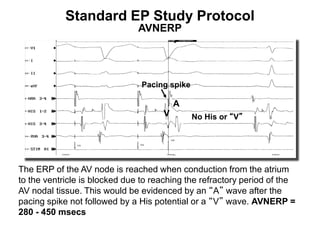
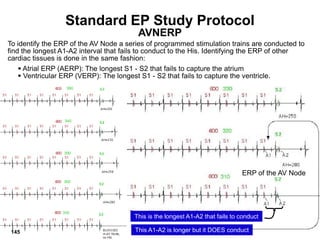
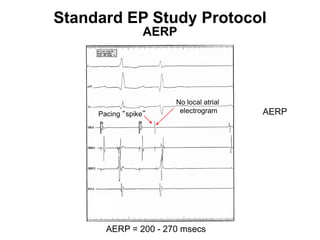
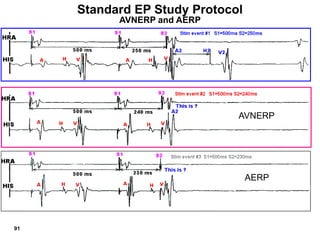
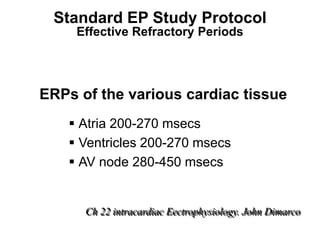
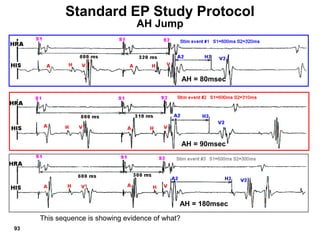
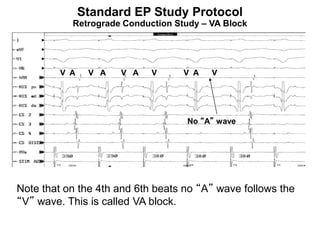
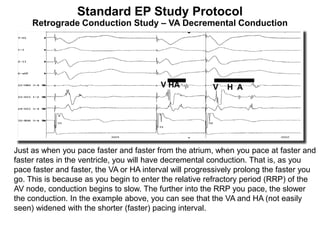
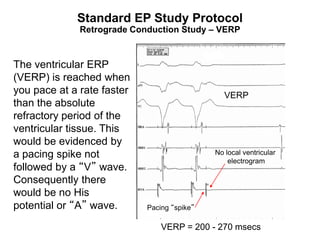
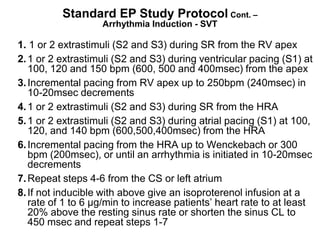
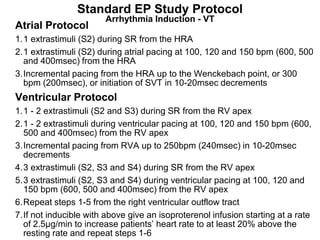
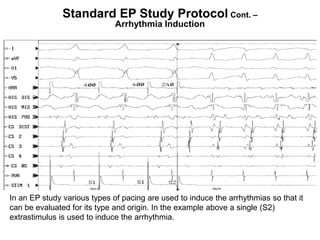
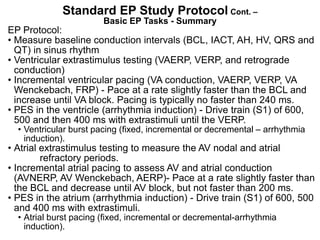

Electrophysiologic studies use pacing techniques like programmed electrical stimulation (PES) to evaluate cardiac properties. PES involves pacing the heart with drive trains and extrastimuli to measure refractory periods, conduction dynamics, and induce arrhythmias. Pacing can be unipolar or bipolar, and incremental, decremental, or with extrastimuli. Refractory periods like the effective refractory period and relative refractory period are measured using premature extrastimuli during pacing. These techniques provide important information about normal cardiac function and arrhythmia mechanisms.




























![EPS part 2 FINAL [Autosaved].pptx........](https://cdn.slidesharecdn.com/ss_thumbnails/epspart2finalautosaved-250127140443-78c2d1e9-thumbnail.jpg?width=640&height=640&fit=bounds)

















![ECG & Heart block [doctors online]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgheartblockdoctorsonline-131111054313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)







































