Downloaded 24 times

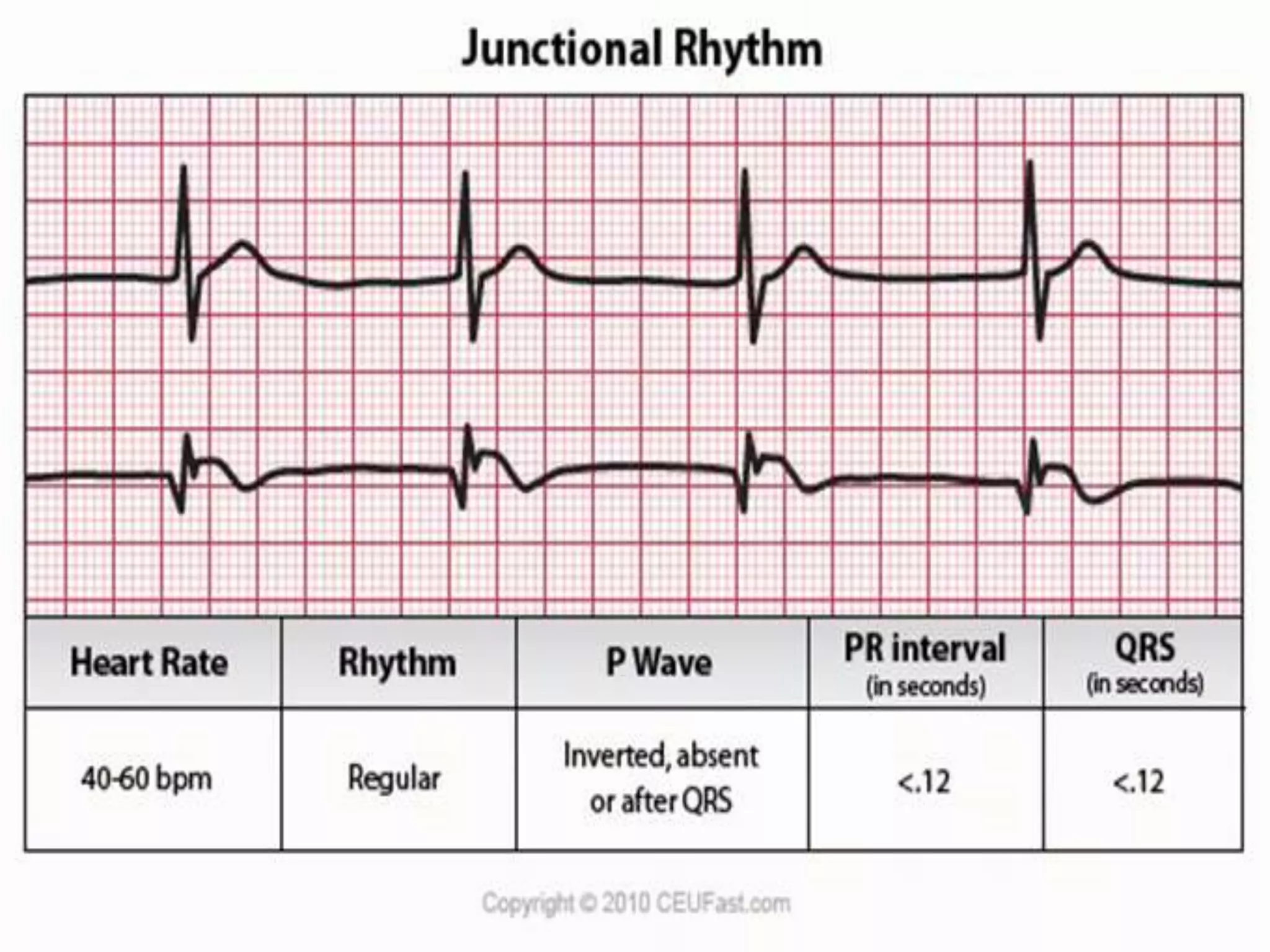































































This document provides information on various cardiac dysrhythmias, including their causes, types, and management. It discusses junctional rhythms arising from the AV junction and their two major types - disturbances in automaticity and disturbances in conduction. Various types of AV blocks are described including first, second (Mobitz I and II), and third degree heart block. Other arrhythmias covered include bundle branch blocks, ventricular arrhythmias, pre-excitation syndromes like Wolf-Parkinson-White syndrome, and sudden cardiac death. The management of dysrhythmias through pharmacotherapy, defibrillation, ablation, and pacemakers is also summarized.






































![Dysrhythmia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysrhythmiaautosaved-230617180733-e317f7a6-thumbnail.jpg?width=640&height=640&fit=bounds)
















































