Downloaded 39 times



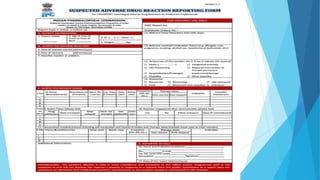



Pharmacovigilance is the science of monitoring drug safety. It began in the 1960s after the thalidomide tragedy caused birth defects. The goal is to detect adverse drug reactions and prevent patient harm. In India, the Pharmacovigilance Programme of India collects ADR reports and analyzes them to inform regulatory decisions. Healthcare professionals and patients can report any suspected ADR to regional monitoring centers or the national helpline. Collecting ADR data helps ensure medications have favorable benefit-risk profiles.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









