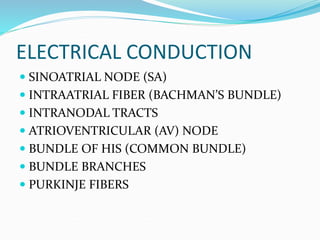
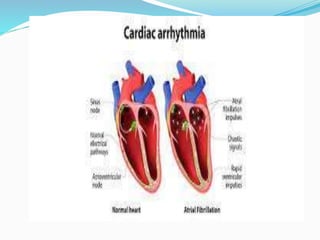
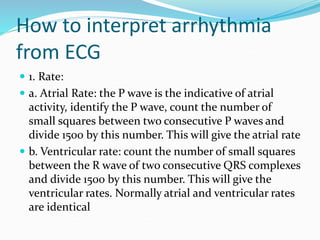
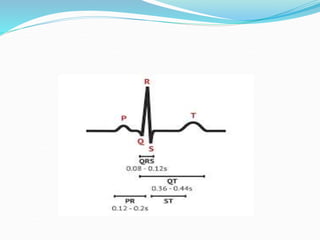
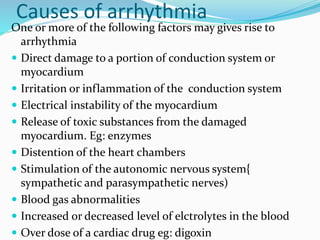
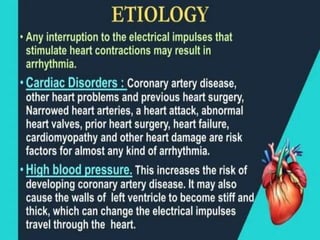
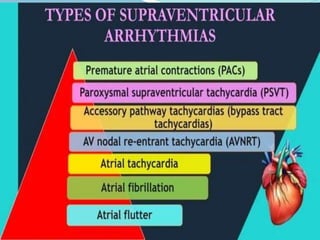
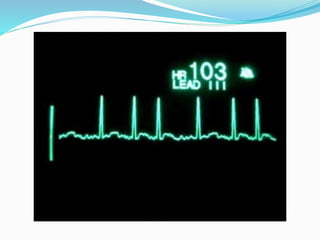
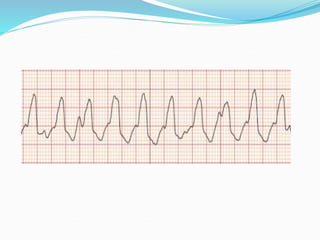
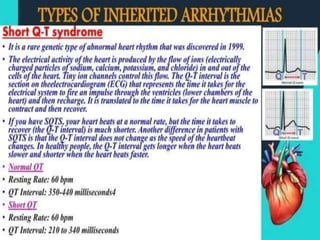
An arrhythmia is an irregular heartbeat that occurs when the heart's electrical signals don't work properly, causing the heart to beat too fast, too slow, or irregularly. Some key types discussed include sinus tachycardia, sinus bradycardia, premature atrial contractions, atrial flutter, atrial fibrillation, supraventricular tachycardia, ventricular tachycardia, and heart block. Causes can include direct damage to the conduction system, inflammation, electrolyte imbalances, and drugs. Treatment depends on the specific type but may include medications, catheter ablation, cardioversion, or pacemaker implantation.






































![Dysrhythmia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysrhythmiaautosaved-230617180733-e317f7a6-thumbnail.jpg?width=640&height=640&fit=bounds)


















































