Download as PDF, PPTX
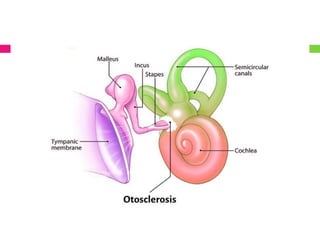
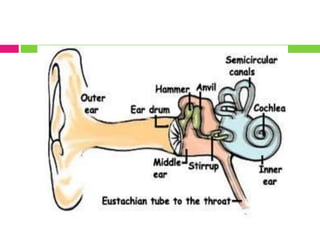
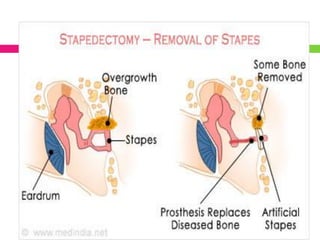


Otosclerosis is a condition where abnormal bone growth occurs on the stapes in the middle ear, causing it to become fixed and preventing sound vibration transmission. This results in conductive hearing loss. It usually affects both ears and causes progressive hearing loss. It has two classifications - histological (found postmortem) and clinical (three subtypes based on location). The exact cause is unknown but heredity is a factor. Symptoms include hearing loss, dizziness, tinnitus, and vertigo. Diagnostic tests include audiometry and imaging. Treatment options include hearing aids and surgery like stapedectomy or stapedotomy to restore hearing. Complications can include infection, dizziness, or deafness























































































