Downloaded 627 times

![cardiac resynchronization therapy
[CRT])
• Biventricular pacing -With this approach, in
addition to single- or dual-chamber right heart
pacing leads, a lead is advanced to the
coronary sinus for left ventricular epicardial
pacing.](https://image.slidesharecdn.com/managementofapatientwithpacemaker-160526174915/75/Management-of-a-patient-with-pacemaker-33-2048.jpg)
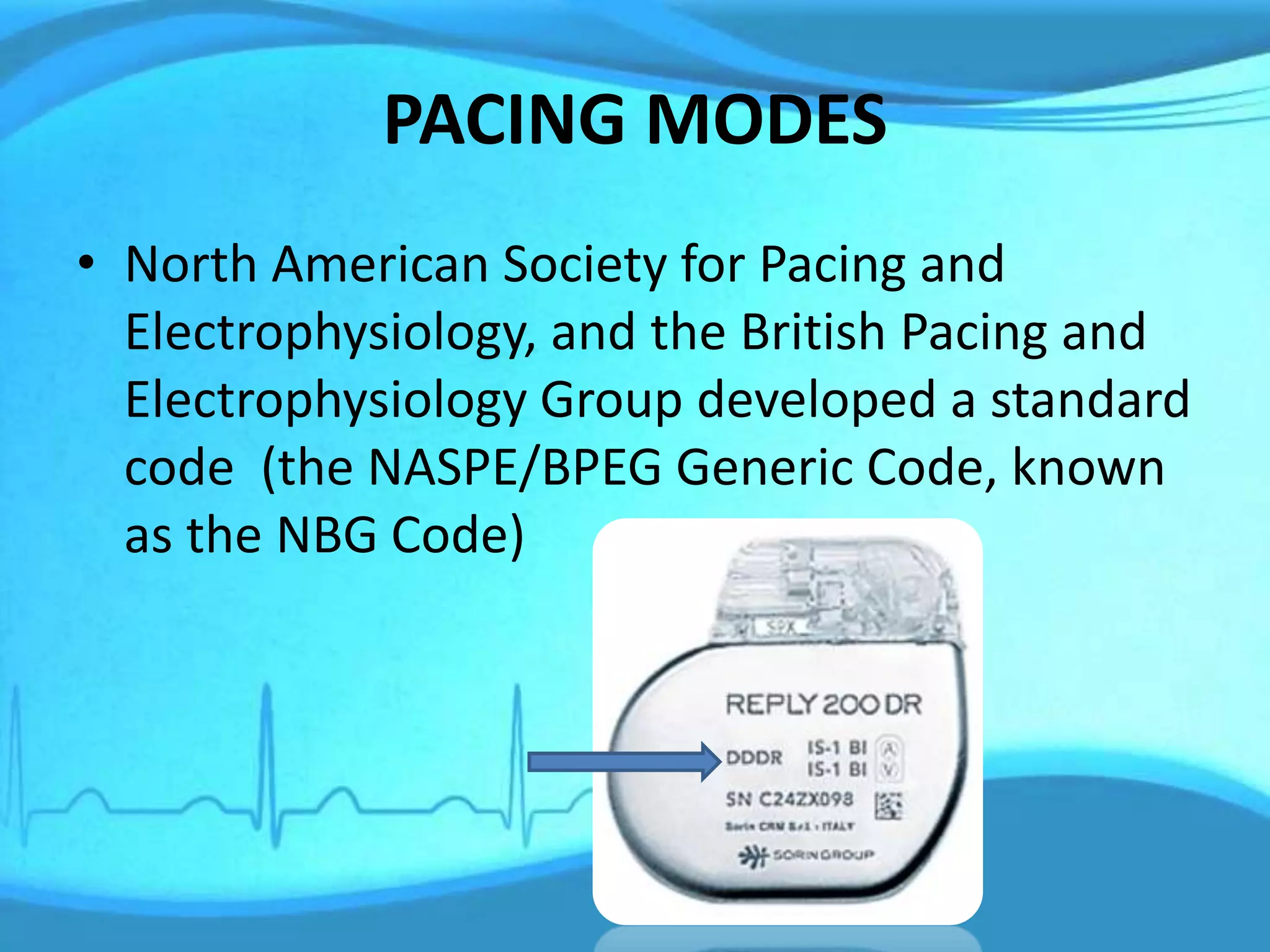





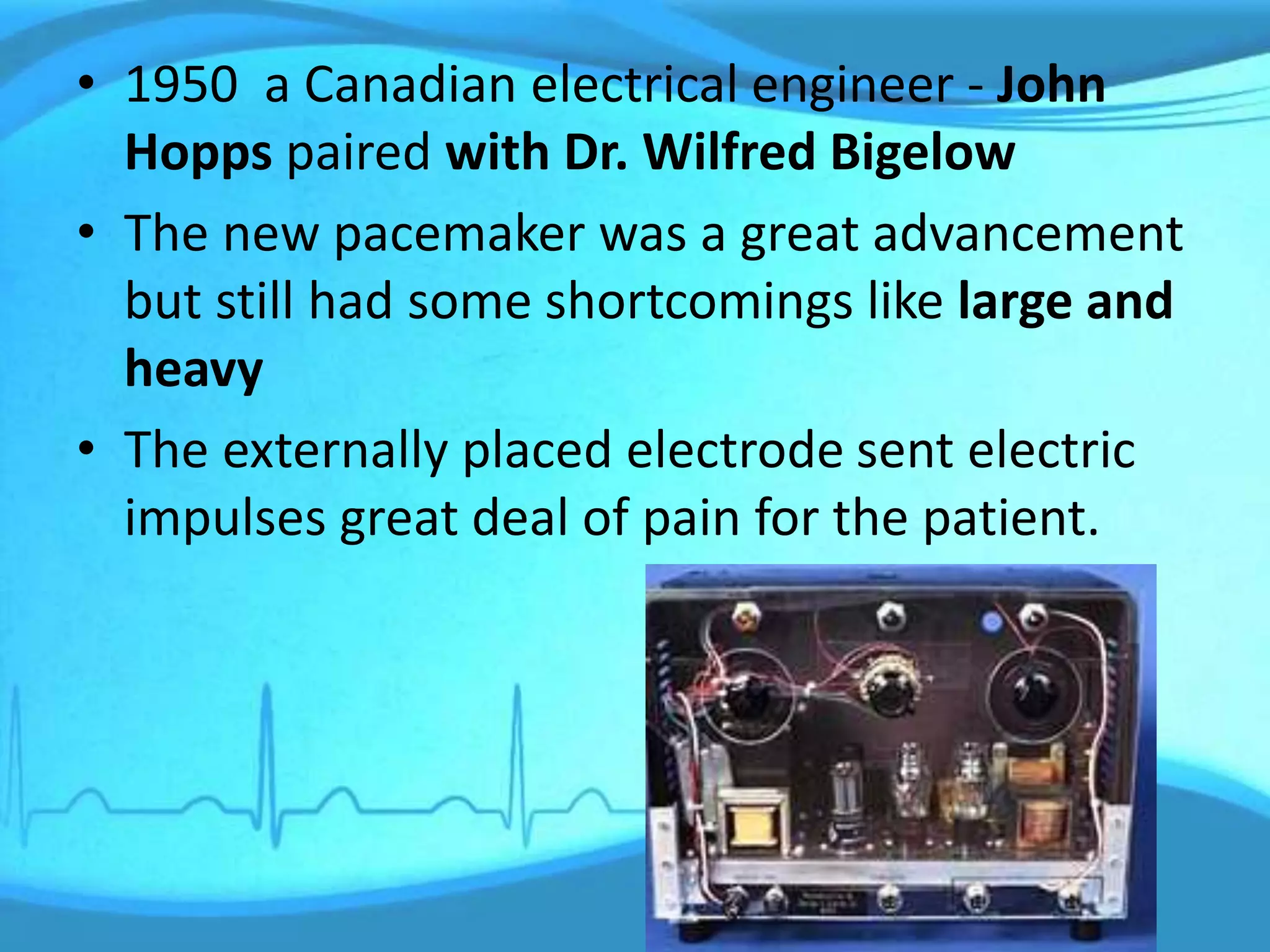
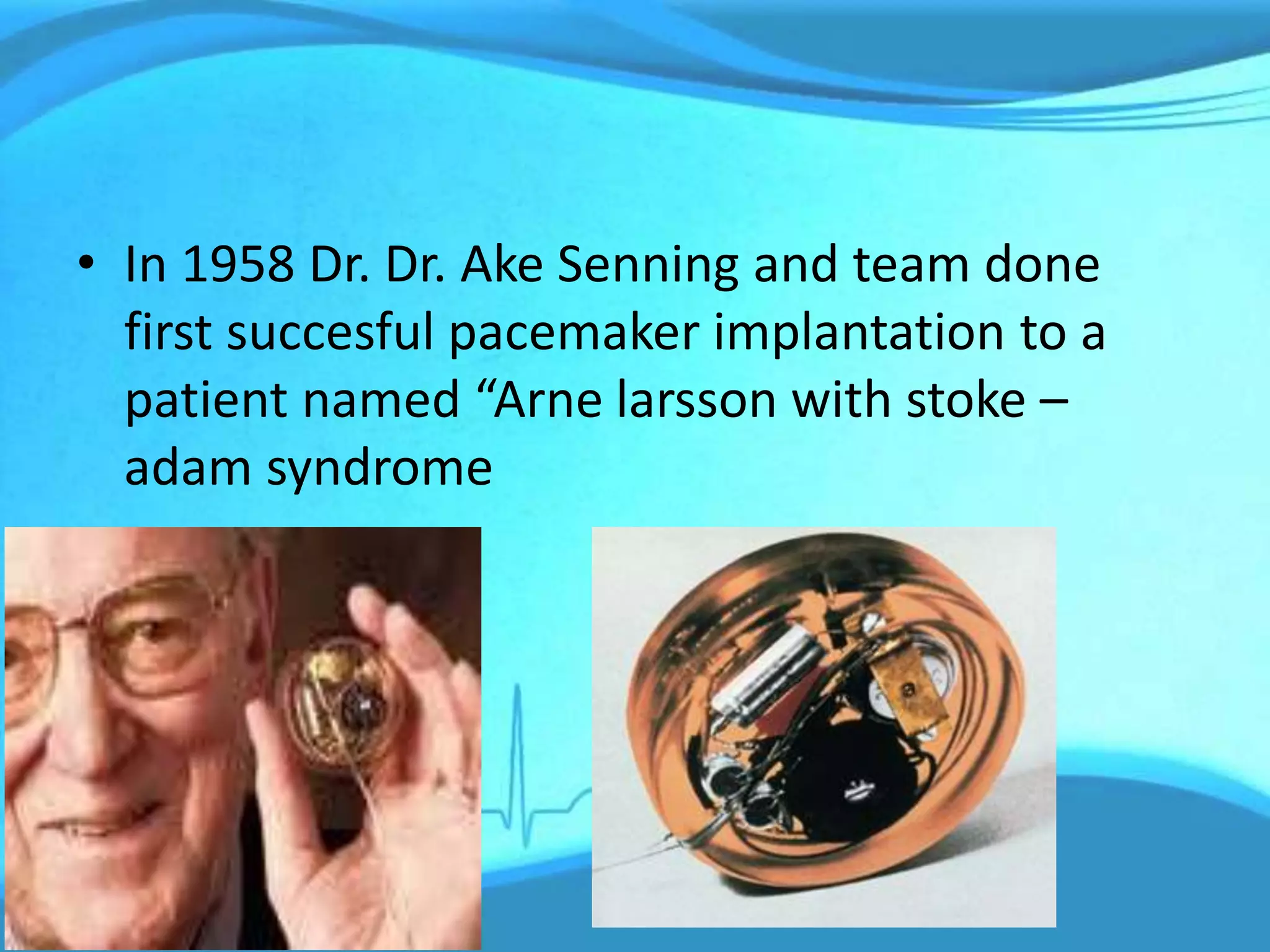
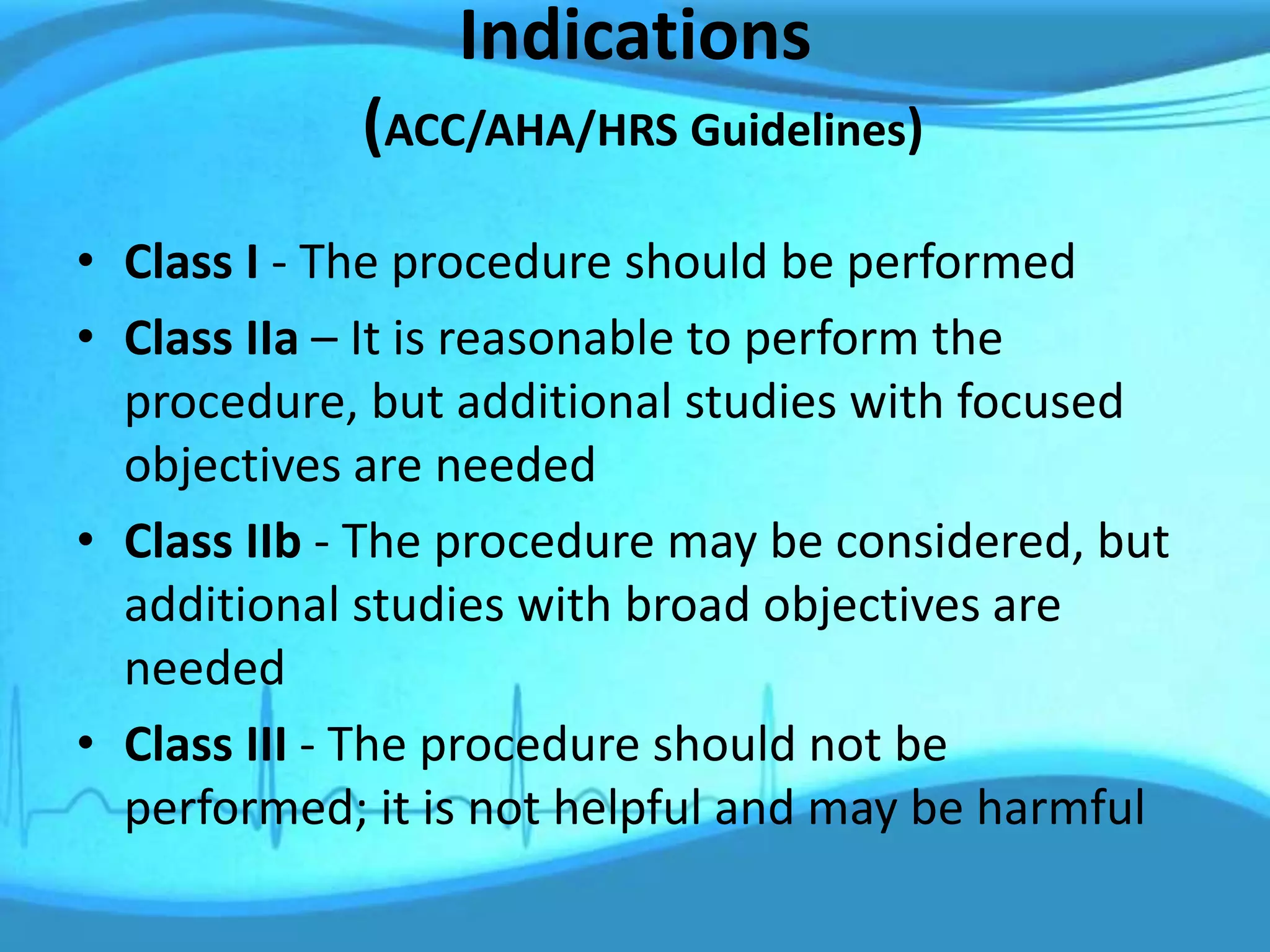
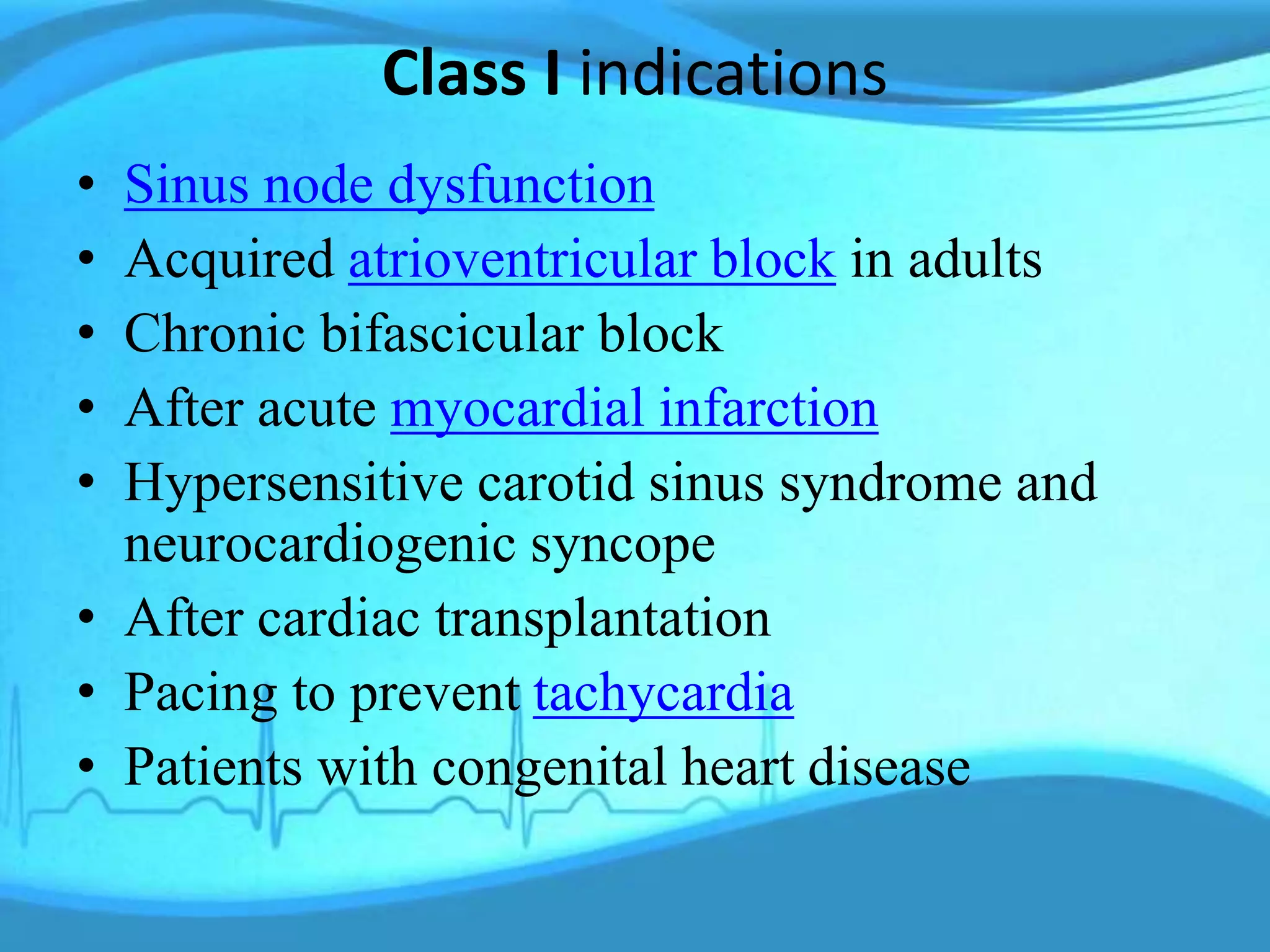
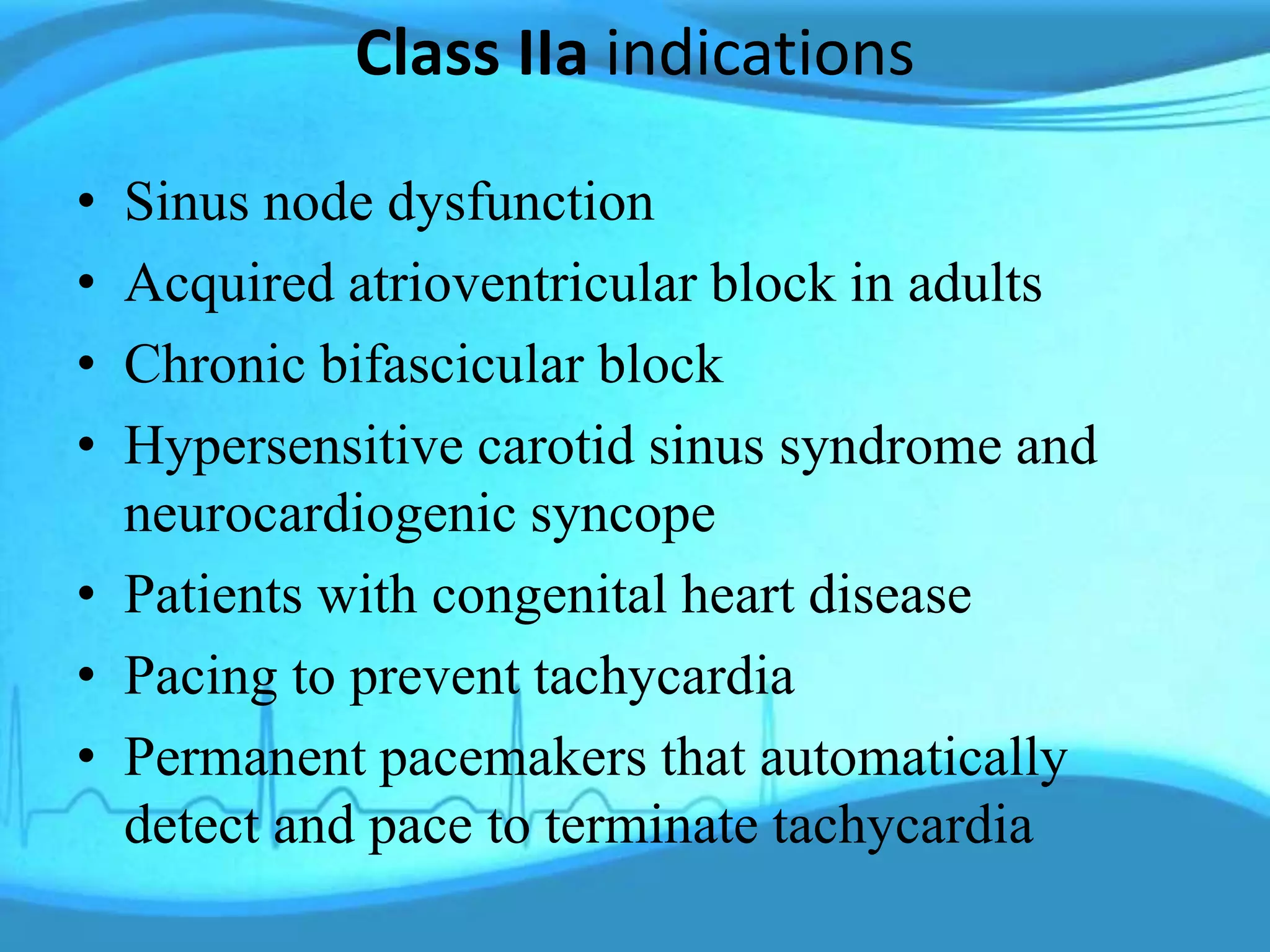
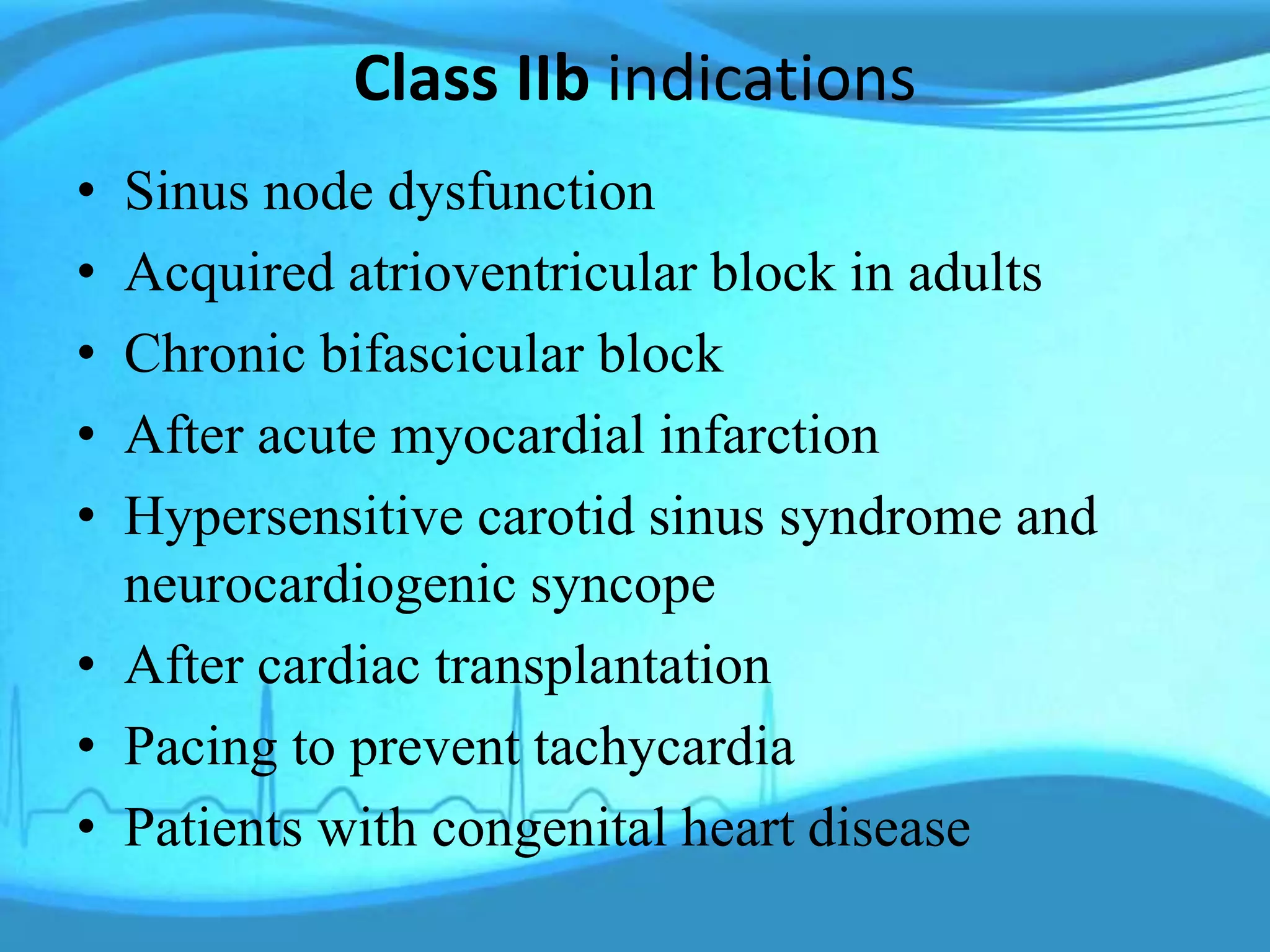
A pacemaker is a medical device that uses electrical pulses to regulate an abnormal heart rhythm. The first pacemaker was implanted in 1958. Modern pacemakers are battery-powered and implanted surgically. They have leads placed in the heart to sense the heart's rhythm and deliver electrical pulses when needed. Pacemakers are programmed to pace one or both chambers of the heart and can inhibit or trigger pacing. Common indications include sinus node dysfunction and heart block. Pacemaker implantation involves accessing a vein, placing leads in the heart, testing the leads, securing the pacemaker generator, and closing the incision. Complications can include bleeding, infection, and lead issues.






















































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)














