Download to read offline


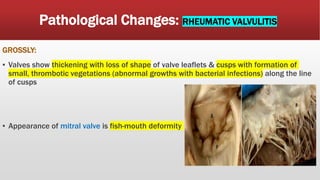
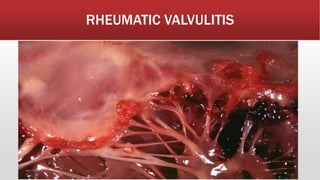
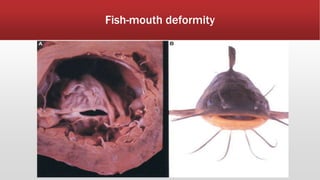
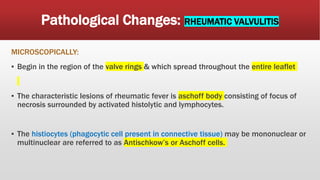
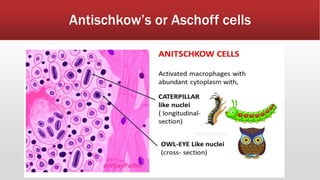


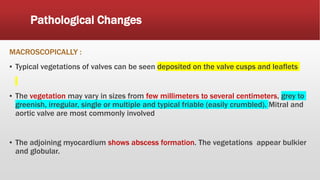
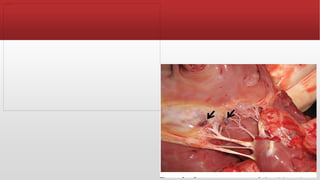
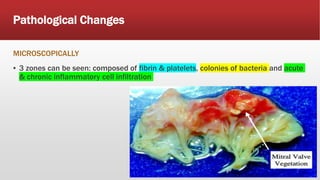

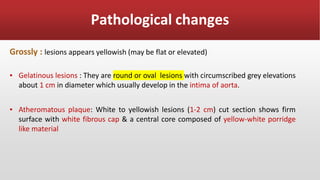
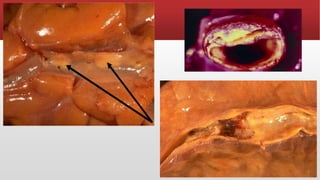



This document describes several pathological changes seen in cardiovascular conditions: 1. Pericardial effusion results in fluid accumulation in the pericardial sac due to non-inflammatory or inflammatory causes. Rheumatic heart disease damages heart valves permanently due to GABHS bacteria. 2. Rheumatic valvular lesions show thickened, deformed valves with thrombotic vegetations and Aschoff cells consisting of necrosis surrounded by lymphocytes. Infective endocarditis shows typical valve vegetations and myocardial abscesses. 3. Atherosclerosis plaques appear yellowish and firm, microscopically showing layers of cells, lipid, and connective tissue. Infarctions appear white




















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)