1) A defibrillator is a device that delivers a therapeutic electrical shock to the heart to treat life-threatening abnormal heart rhythms called fibrillations.
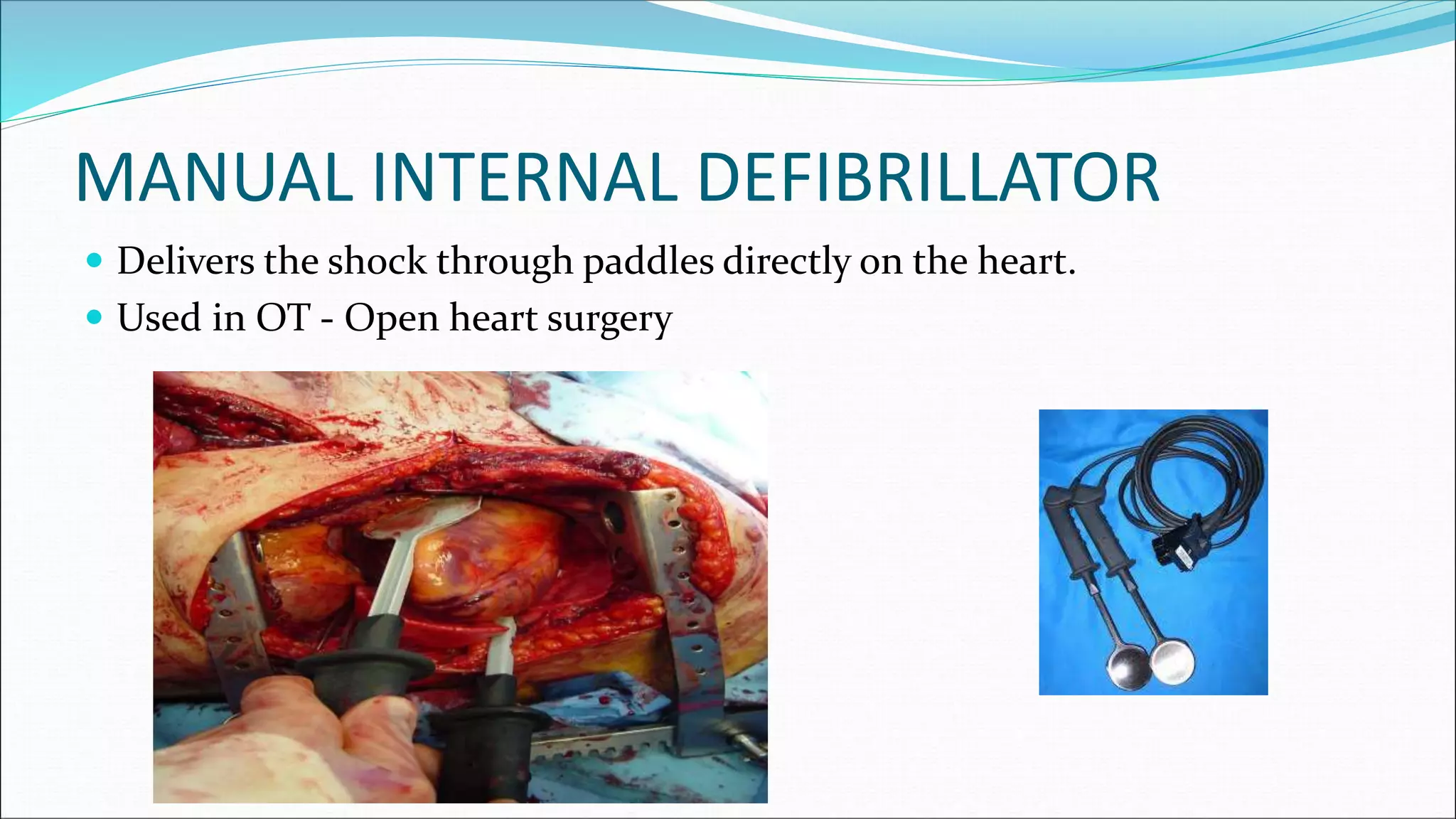
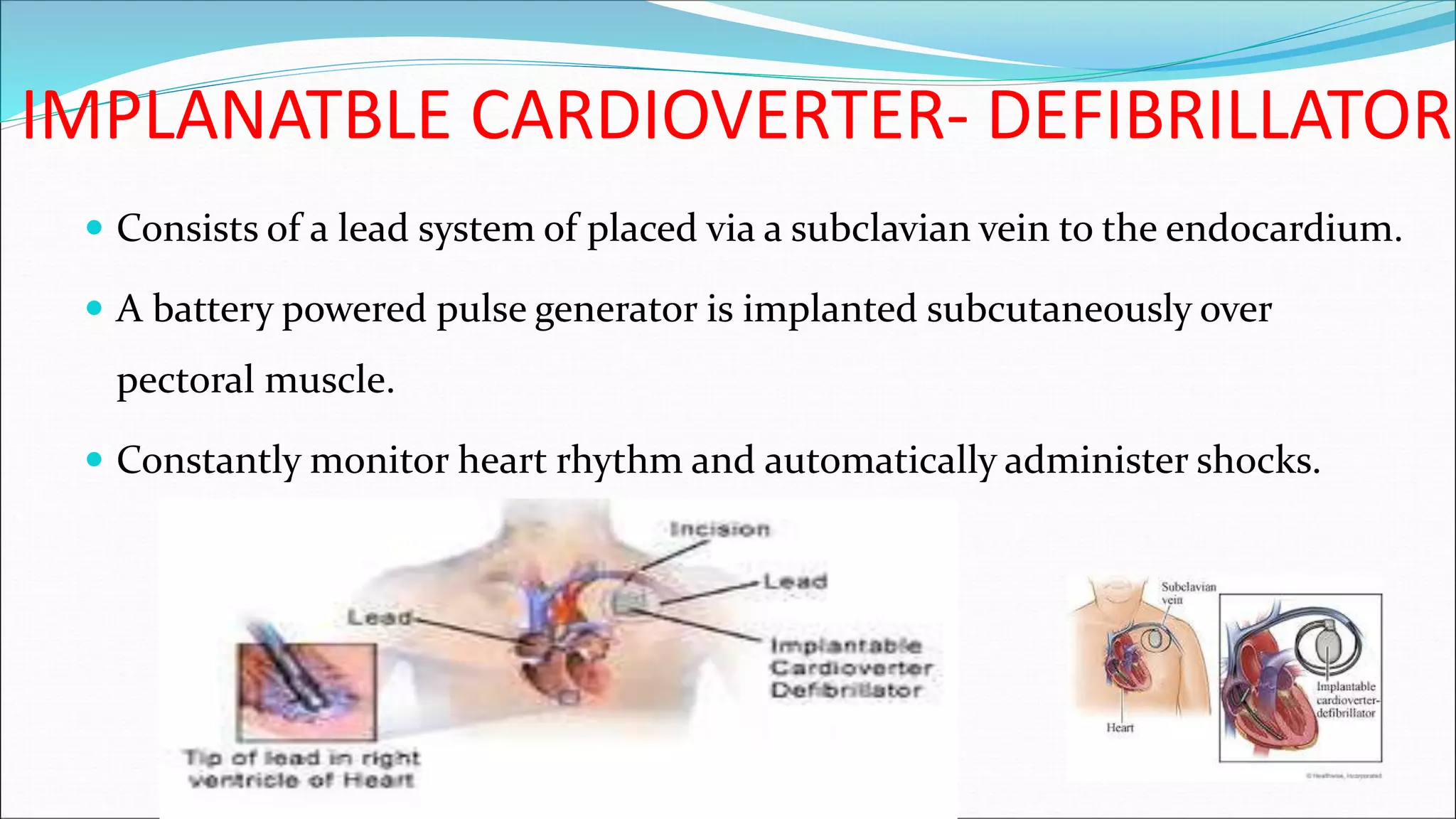
2) There are several types of defibrillators including manual external defibrillators, automated external defibrillators (AEDs), implantable cardioverter-defibrillators, and wearable defibrillators.
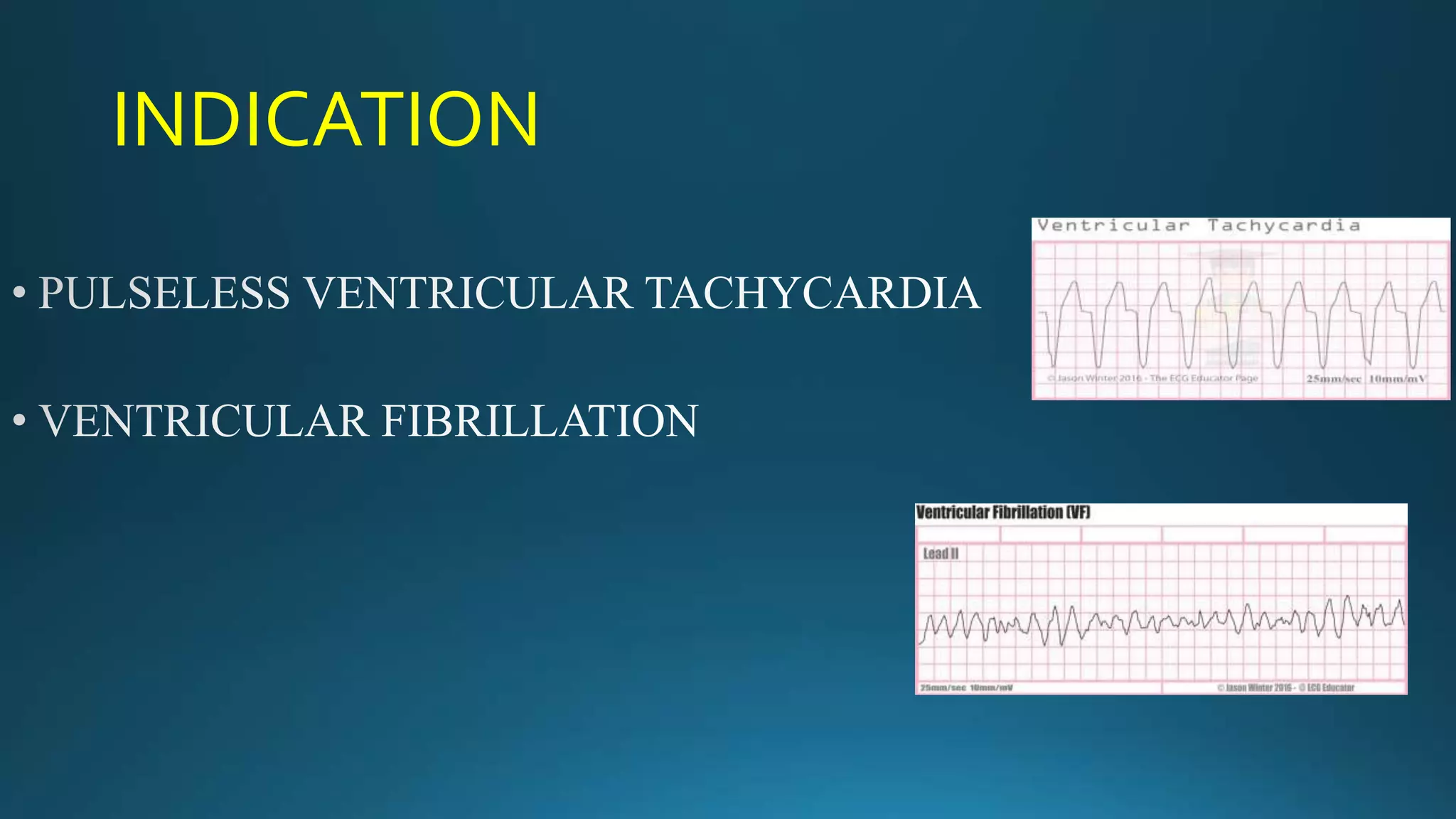
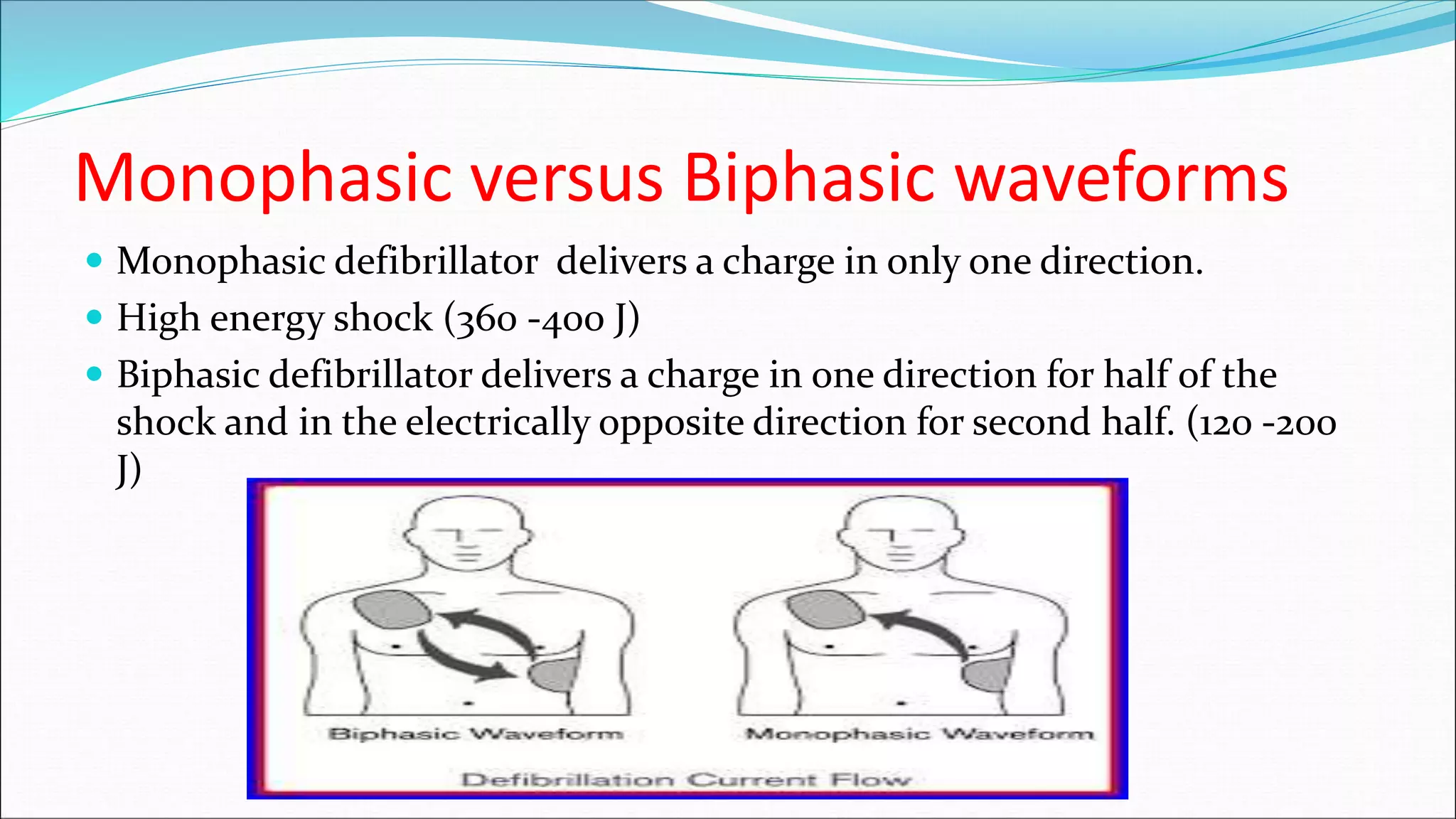
3) The defibrillation process involves assessing the patient's heart rhythm, delivering a controlled electric shock to depolarize the heart and allow the natural pacemaker to resume normal rhythm, then continuing care which may involve further shocks or CPR depending on the patient's response.




































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)







