Downloaded 281 times

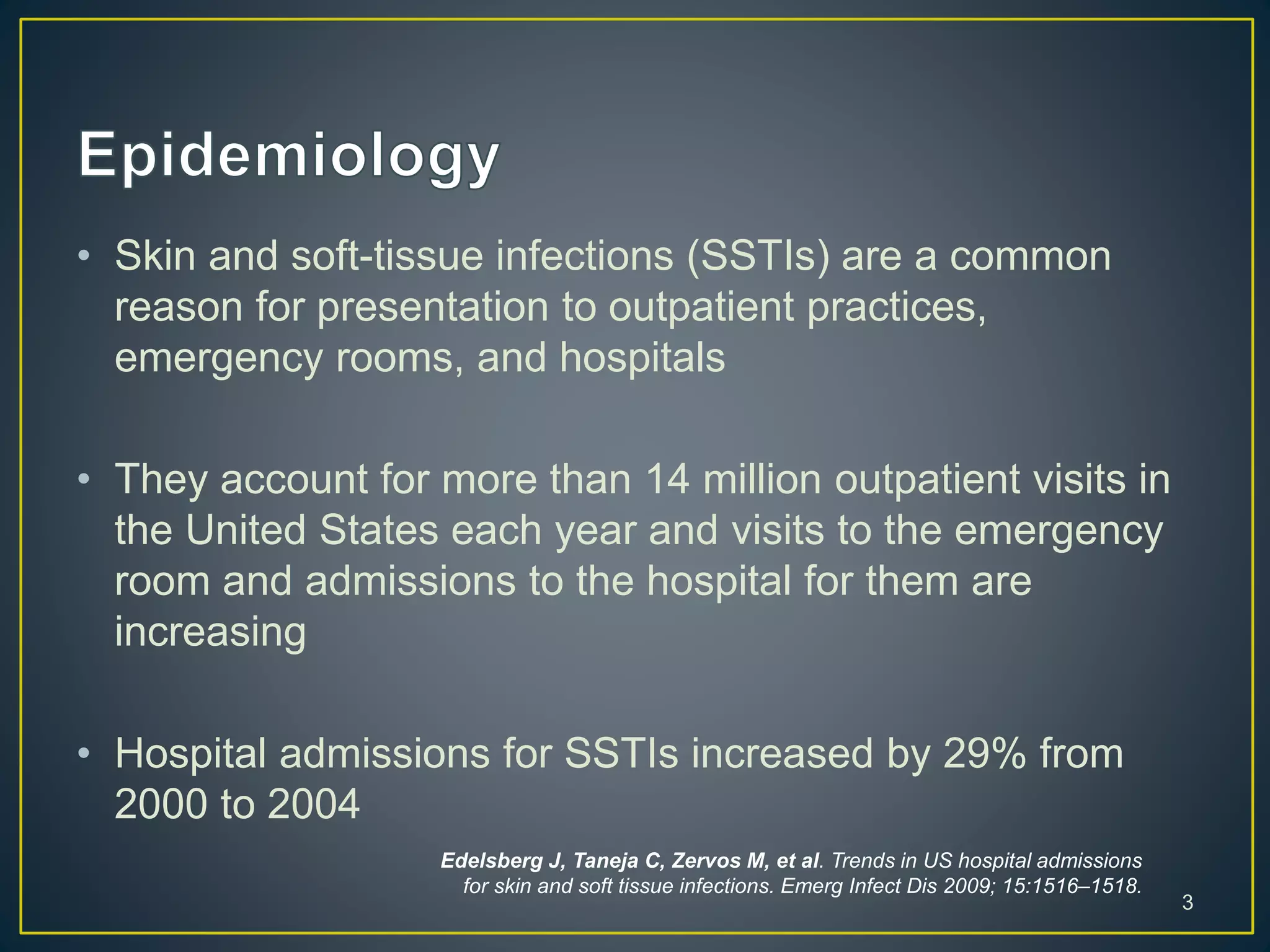

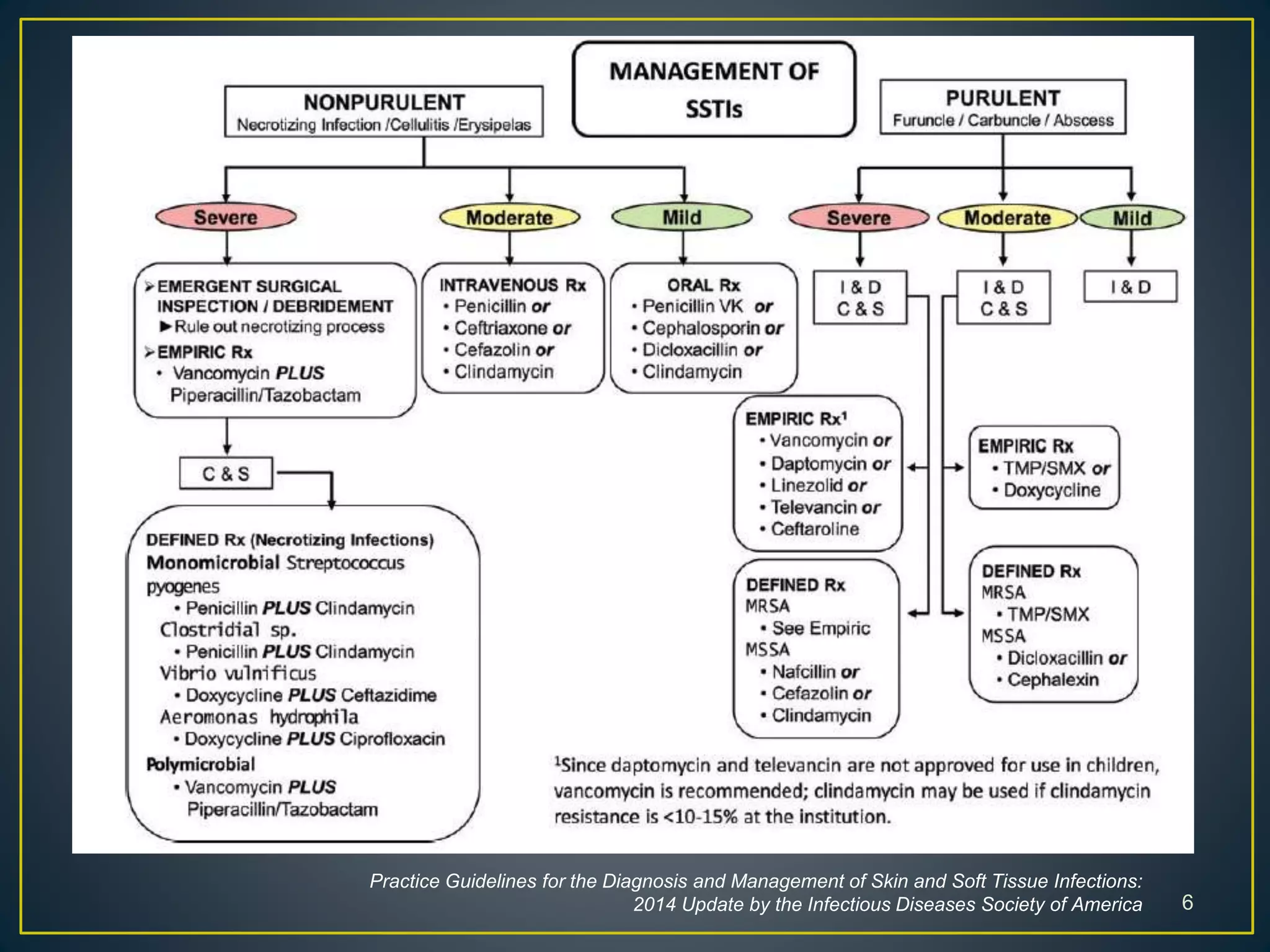





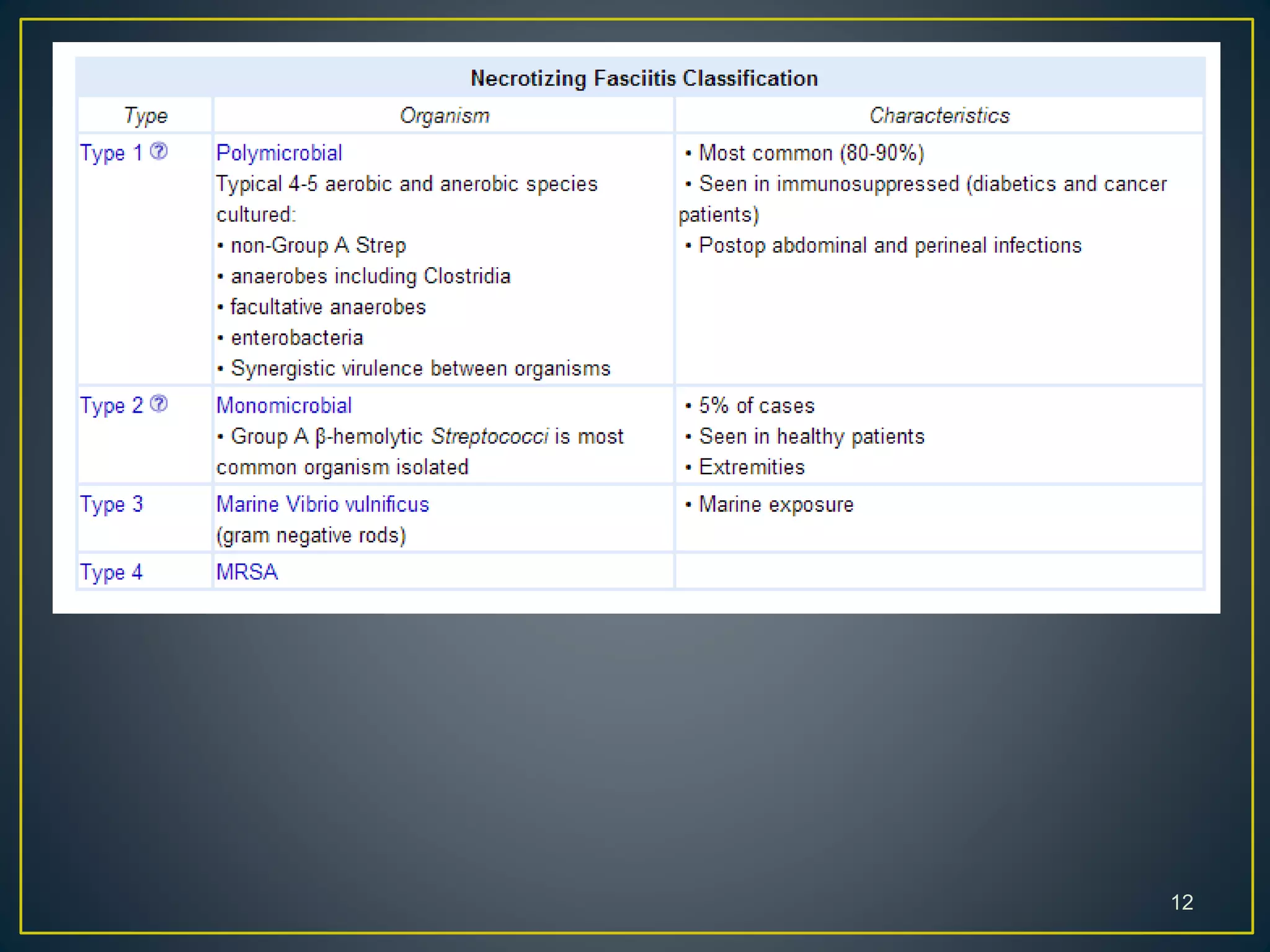



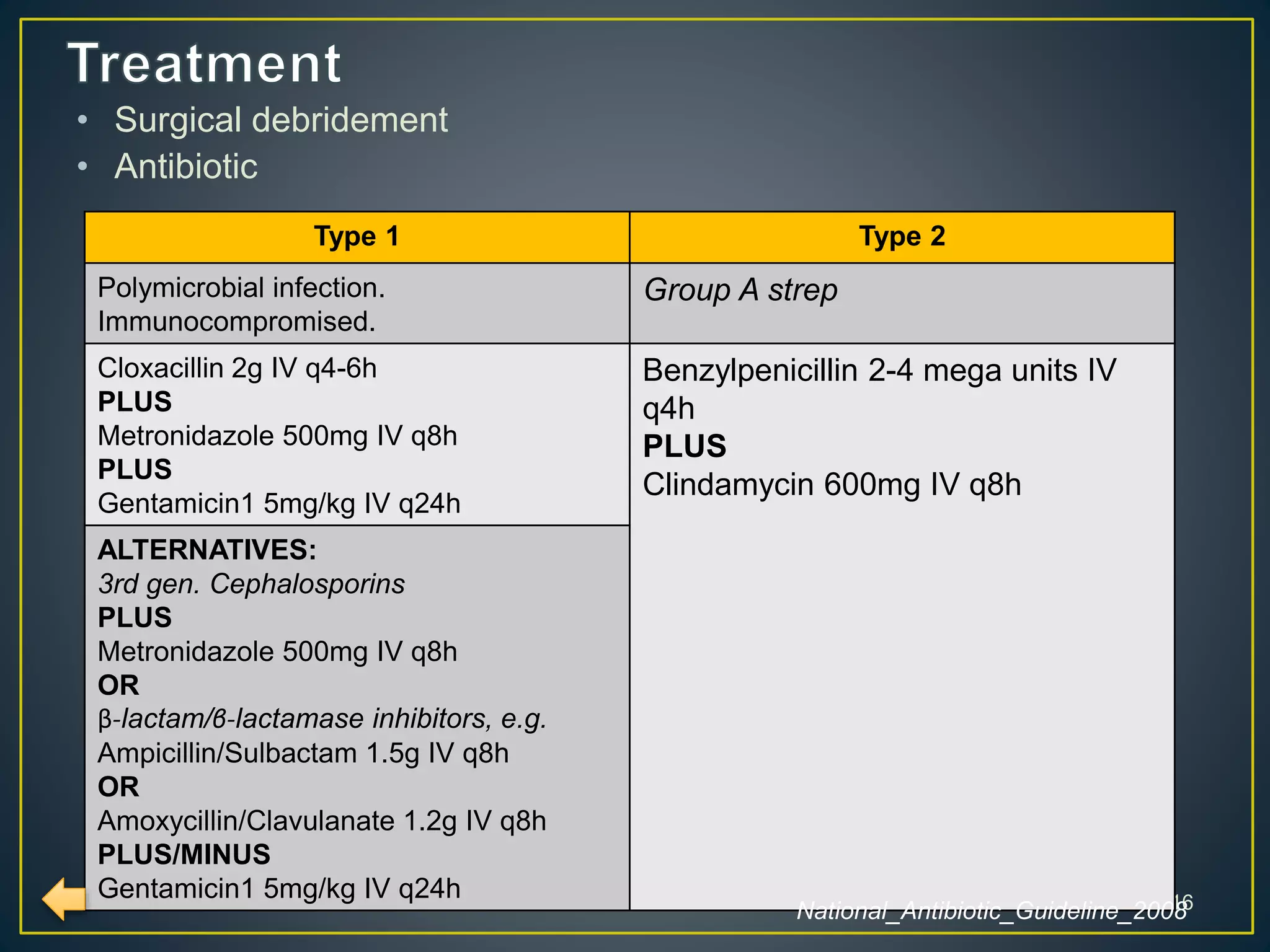



Skin and soft-tissue infections are common reasons for medical visits and hospital admissions in the US. This document discusses different types of skin and soft tissue infections like cellulitis, erysipelas, and necrotizing fasciitis. It provides details on symptoms, indications for admission, diagnostic features, and treatment recommendations for various infections.






























![1.1.1. bacterial infection of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-1-bacterialinfectionofskincompatibilitymode-130325014737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)