Downloaded 644 times
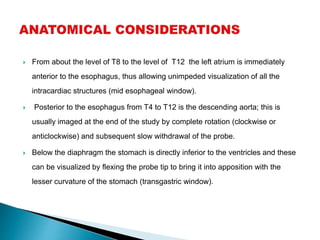
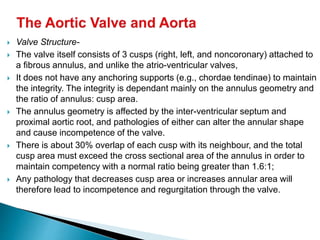
![ The coronary ostia are well seen in the mid esophageal AV short
(left [LCA] and right [RCA]) and AV long (RCA) axis views.
In the SAX view the left main stem (LMS) and proximal portion of
the anterior descending (LAD) and circumflex (LCx) branches can
be seen](https://image.slidesharecdn.com/transesophagealechocardiography-200323104323/85/Transesophageal-echocardiography-TEE-85-320.jpg)


Dr. Awadhesh Kumar Sharma is a distinguished interventional cardiologist with extensive academic and professional credentials, including gold medals in his studies and multiple prestigious awards. He has performed over 10,000 invasive cardiac interventions and is actively involved in teaching and publishing in his field. Currently, he serves as an assistant professor at LPS Institute of Cardiology in Kanpur, focusing on both invasive and non-invasive cardiology techniques.























































































