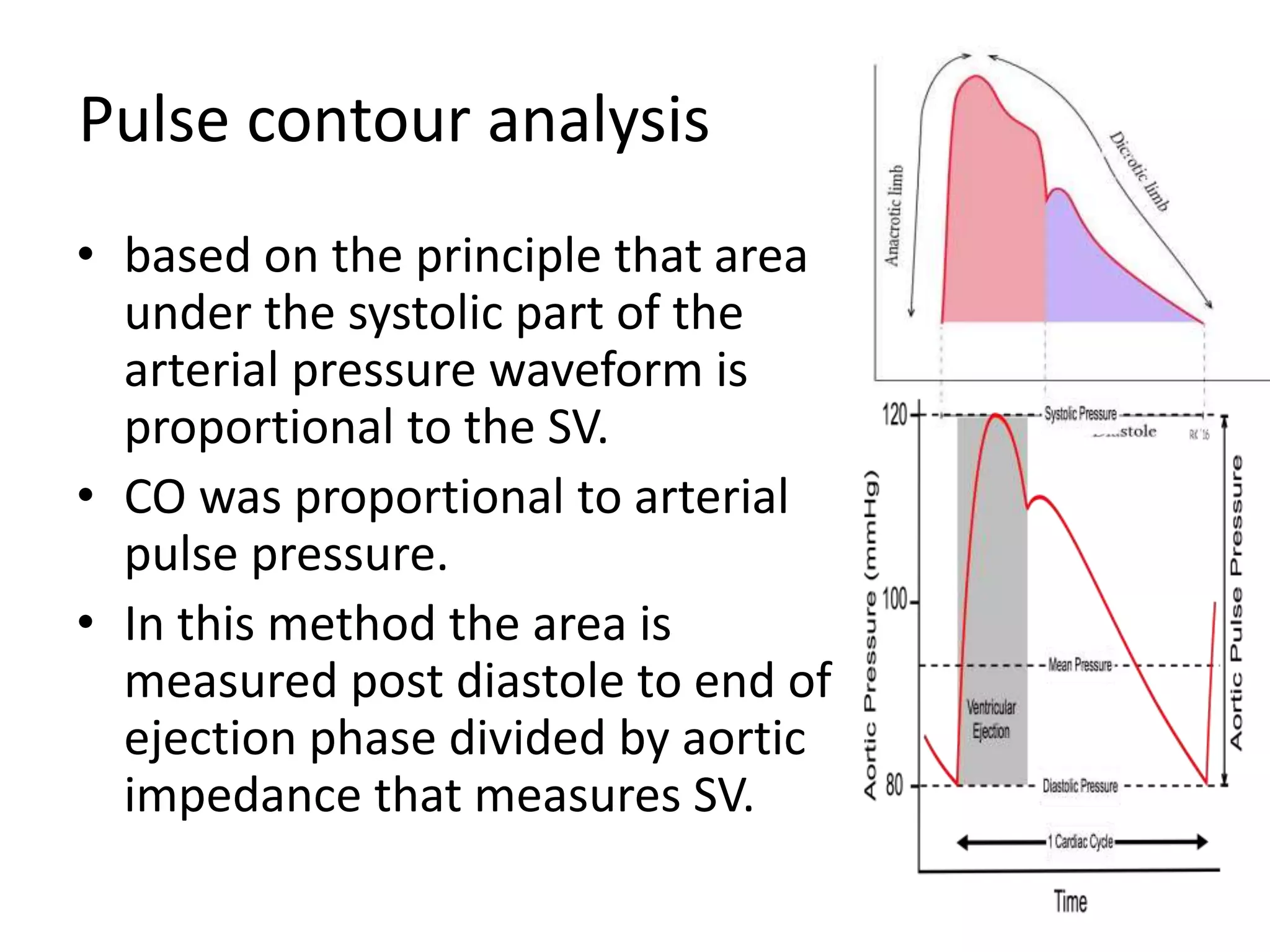
Cardiac output can be measured through various invasive and non-invasive methods. The pulmonary artery catheter using thermodilution is still considered the gold standard but is invasive. Minimally invasive methods include lithium dilution, pulse contour analysis devices, esophageal Doppler, and transesophageal echocardiography. Non-invasive methods include partial gas rebreathing, thoracic bioimpedance, and Doppler ultrasound. The ideal monitor is accurate, continuous, non-invasive and provides reliable measurements during different physiological states.