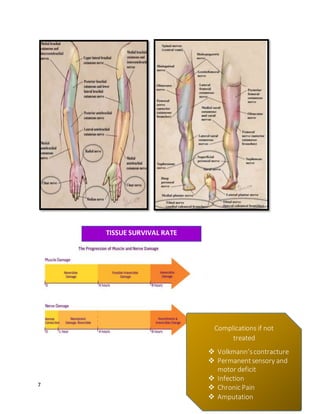
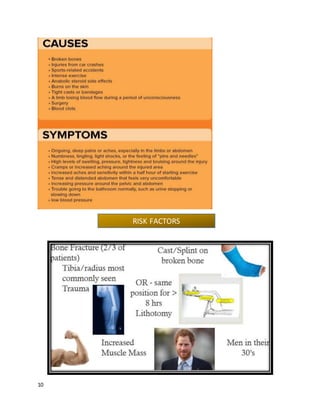
Compartment syndrome is a serious condition caused by increased pressure within the fascial compartments of the body that can compromise blood flow. It requires immediate medical attention to prevent permanent muscle and nerve damage. The condition is diagnosed based on severe pain out of proportion to the injury that is worsened with stretching of the affected muscles. Treatment involves surgical fasciotomy to release the pressure within the compartments. Early diagnosis and treatment are essential to avoid long-term complications.