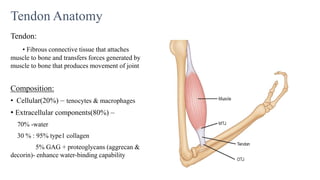
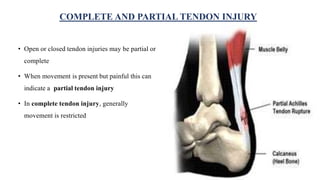
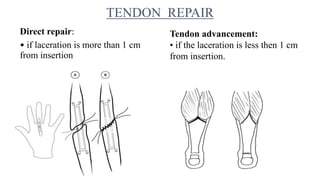
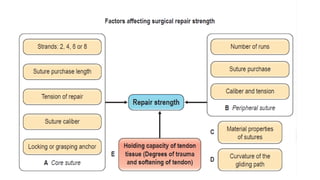
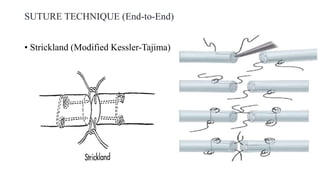
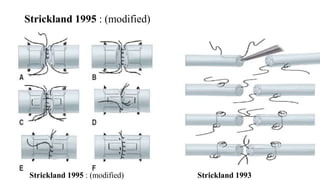
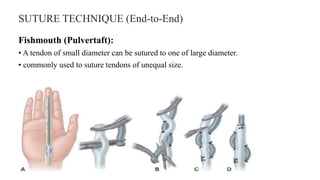
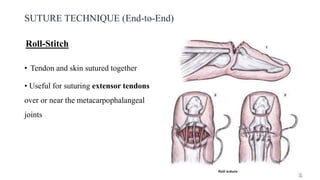
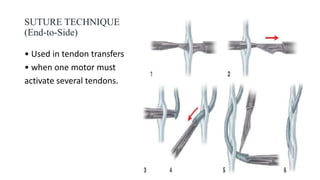
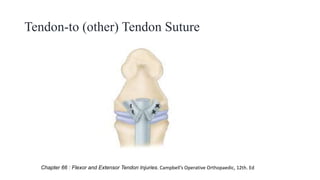
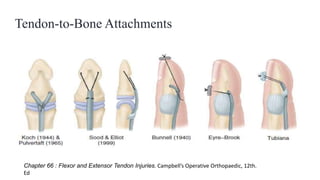
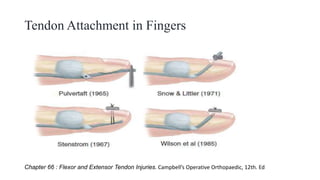
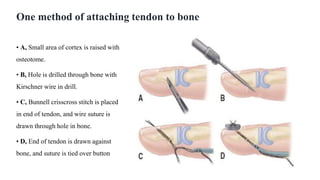
This document discusses tendon anatomy, injury, and repair. It describes the composition and vascular supply of tendons. Common tendon injuries include open wounds requiring surgical repair and closed injuries causing deformities. The goals of repair are to reestablish tendon continuity and gliding function. Various suture techniques are discussed for end-to-end, end-to-side, and tendon-to-bone repairs. Post-operative rehabilitation aims to promote intrinsic healing while minimizing scarring through early controlled motion to optimize tendon gliding and range of motion recovery.





















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
