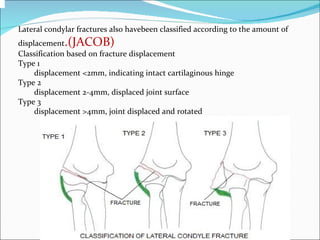
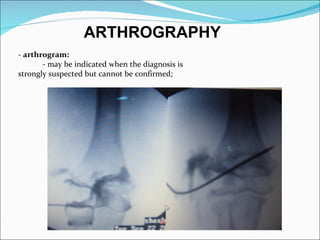
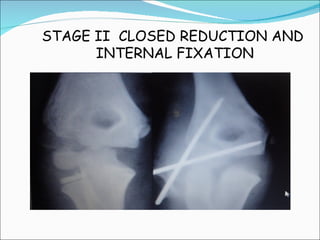
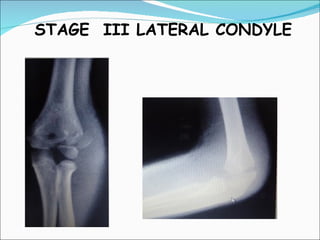
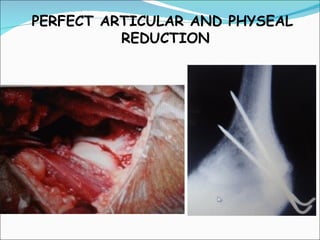
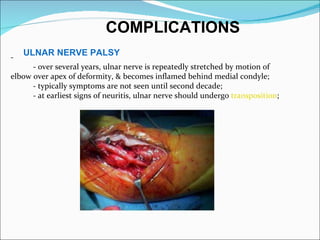
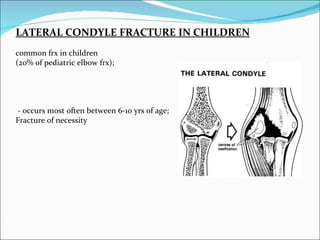
Lateral condyle fractures of the elbow are common in children between ages 6-10 years. They occur when a varus force is applied to an extended elbow. These fractures are prone to displacement and nonunion due to pull from forearm extensors and being bathed in synovial fluid. Treatment depends on the amount of displacement, with undisplaced fractures often treated non-operatively and displaced fractures requiring closed or open reduction and internal fixation. Complications can include ulnar nerve palsy, osteonecrosis, nonunion, and cubitus deformities.
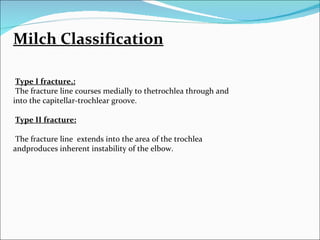
![Figure 2Illustrations of the Milch classification of lateral condylar fracture.
A, In type I, the fracture line courses lateral to the trochlea and exits into the
capitulotrochlear groove.
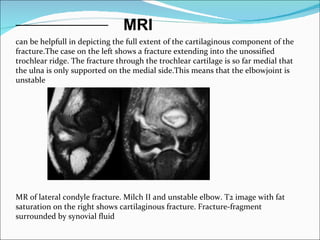
B, In type II, the fracture line extends into the apex of the trochlea.
(Reproduced from Sullivan JA: Fractures of the lateral condyle of the humerus.
J Am Acad Orthop Surg 2006;14[1]:58-62.)](https://image.slidesharecdn.com/finalfinalmadhusir-120715112820-phpapp01/85/Final-final-madhu-sir-9-320.jpg)