Chronic limb ischemia
•Download as PPTX, PDF•
32 likes•7,146 views

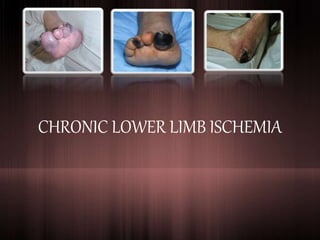
Chronic critical limb ischemia is manifested by pain at rest, nonhealing wounds and gangrene. Ischemic rest pain is typically described as a burning pain in the arch or distal foot that occurs while the patient is recumbent but is relieved when the patient returns to a position in which the feet are dependent

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Chronic limb ischemia
Similar to Chronic limb ischemia (20)
More from Dr Slayer
More from Dr Slayer (15)
Recently uploaded
Recently uploaded (20)
Chronic limb ischemia
- 1. CHRONIC LOWER LIMB ISCHEMIA
- 2. ANATOMY 1. Aortoiliac segment (inflow) 2. Femoropopliteal segment 3. Infrapopliteal segment (outflow)
- 3. INTRODUCTION • Chronic Limb ischemia = Decrease in limb perfusion > 2 weeks 2007 Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) • Aetiology: Atherosclerosis (90%) • May present at any point along a scale of severity: Mild Intermittent Claudication Rest pain Ischaemic skin changes Gangrene of large part of limb ** 2 distinct entities: Intermittent claudication (IC) Critical Limb Ischaemia (CLI)
- 4. (A) INTERMITTENT CLAUDICATION 5% people over 60 y.o. (only 1-2% deteriorates) Ddx: neurogenic; venous claudication Definition of IC - Muscular pain - Not present at rest - Comes on walking a particular distance (claudication distance) - Quickly relieved by resting - Repetitive Mx: Best Medical Therapy (BMT) – risk factor modification Surgical/endovascular intervention only after 6 month compliance to BMT
- 6. CRITICAL LIMB ISCHEMIA • Multiple lesions affecting different arterial segments • Features: – Rest pain – Tissue loss (ulcer/gangrene) – Low Ankle Brachial Pressure Index (<0.5) • Fontaine III & IV
- 7. ISCHEMIC ULCERS VENOUS ULCERS PAIN Yes, unless neuropathic Minimal; not intolerable DURATION Less than 6 weeks Often months/years PAST HISTORY Cardiac ischemia/CABG common DVT/ severe varicose veins LIMB SIGNS SWELLING Not swollen unless pt has been sleeping in a chair to relieve pain Usually non-pitting plus pitting edema unless effective bandaging in place TEMPERATURE Usually cold Usually normal or warm PULSES Absent; low Doppler pressure *ABSI/ABPI Present; normal Doppler pressure ULCERS SITE Toes, dorsum of foot Gaiter’s area MARGIN Punched out Irregular with blue margin & growing epithelium BASE Destroy deep fascia & may expose tendons, with poor granulation Beefy red, shallow and never penetrate deep fascia, pale granulation tissue
- 8. MANAGEMENT NON- SURGICAL MANAGEMENT Pharmaco Non-pharmaco SURGICAL MANAGEMENT Minimally invasive Invasive Stop smoking Hypertension control Hypercholester olemia control Antiplatelet agent Regular exercise Obesity control Diabetes identification & active treatment Foot care Best Medical Therapy (BMT) -endaarterectomy -Balloon angioplasty with/without stenting -Bypass surgery (arterial reconstruction) - Amputation
- 10. Buerger’s Disease Non-atherosclerotic, idiopathic, recurrent, segmental inflammatory, vasculopathy of medium & small sized arteries & veins of upper & lower extremities Diabetic Foot Combination of ischemia, neuropathy, & immunocompromise that renders the feet of diabetic pt susceptible to sepsis, ulceration & gangrene. Challenges in diabetic vascular disease: - Calcified - Reduce ability to fight infection - Multisystem - Infrapopliteal vessels - Co-existing neuropathy
- 11. REFERENCES • Principles & Practice of Surgery • Essentials Surgery • Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II), L. Norgren et. al., Eur J Vasc Endovasc Surg Vol 33, Supplement 1, 2007 • Review Articles: Critical limb ischemia, Varu et. al., Journal of Vascular Surgery, 2010 • Chronic lower limb ischemia, J.D. Beard, BMJ 2000
Editor's Notes
- At 1 year following presentation, 25% of patients have resolved CLI, 20% have ongoing CLI, 30% are alive with amputation, and 25% are dead.1 Therapeutic goals in treating CLI patients include reducing cardiovascular risk factors, relieving ischemic pain, healing ulcers, preventing major amputation, improving quality of life and increasing survival. Symptoms: Ischemic rest pain — A severe decrease in limb perfusion can result in ischemic rest pain due to diffuse pedal ischemia. Ischemic rest pain is typically localized in the forefoot and toes, and is not readily controlled by analgesics. Ischemic rest pain is brought on, or made worse by, elevation of the lower extremity, and is often worse when the patient reclines [20]. The pain can also be felt more proximally, but when this occurs, the pain usually does not spare the foot. Pain can be more localized in patients who develop an ischemic ulcer or gangrenous digits. (See 'Nonhealing wound/ulcer' below and 'Skin discoloration/gangrene' below.) Affected patients frequently find that the pain is relieved by hanging their feet over the edge of the bed, or, paradoxically (in contrast to claudication), by walking around the room because of the gravitational effect of dependence on extremity perfusion. Chronic reductions in extremity blood flow can also lead to a superimposed ischemic neuropathic pain that is frequently described as throbbing or burning, and/or severe shooting pains in the limb. In patients with diabetes, differentiating diabetic neuropathy from combined diabetic ischemic neuropathy can be difficult. (See "Evaluation of the diabetic foot".) Severe diffuse pain — Diffuse acute limb ischemia is characterized by the sudden onset of extremity pain progressing to numbness and finally paralysis of the extremity, accompanied by pallor, paresthesias, coolness, and absence of palpable pulses. In patients with PAD, diffuse ischemia can be due to atheroembolism, thrombotic occlusion of a stenotic artery, or thrombosis of a vascular prior stent or vascular reconstruction [21]. Nonhealing wound/ulcer — Ischemic ulcers often begin as minor traumatic wounds and then fail to heal because the blood supply is insufficient to meet the increased demands of the healing tissue [21]. Ischemic ulcers, which most often involve the foot, can become infected and may lead to osteomyelitis. In patients who are bedbound, lower extremity pressure ulcers can develop, and fail to heal with standard therapies. In patients with diabetes, nonhealing ulcers can develop over points of bony pressure. The general assessment of wounds and special considerations for pressure ulcers and diabetic ulcers are discussed in detail elsewhere. (See "Clinical assessment of wounds" and "Epidemiology, pathogenesis and risk assessment of pressure ulcers" and "Evaluation of the diabetic foot".) Skin discoloration/gangrene — Extremity ischemia alters the appearance of the skin. Patients may notice focal areas of discoloration or skin color changes when their foot is elevated (pale or white) or lowered (redness). If the blood supply falls below what is necessary to meet minimal metabolic requirements, focal areas of ischemia that begin as skin discoloration can progress to full-thickness skin necrosis, which can progress into the deeper tissues [21]. The blue toe syndrome (picture 1), usually due to embolic occlusion of digital arteries with atheroembolic material from a proximal arterial source, may progress to a nonhealing ulcer or focal areas of gangrene if severe PAD is present.
- 3 prerequisites for reconstruction Good inflow Suitable conduit Good outflow
- Buerger’s main mx: quit smoking