Download as PDF, PPTX



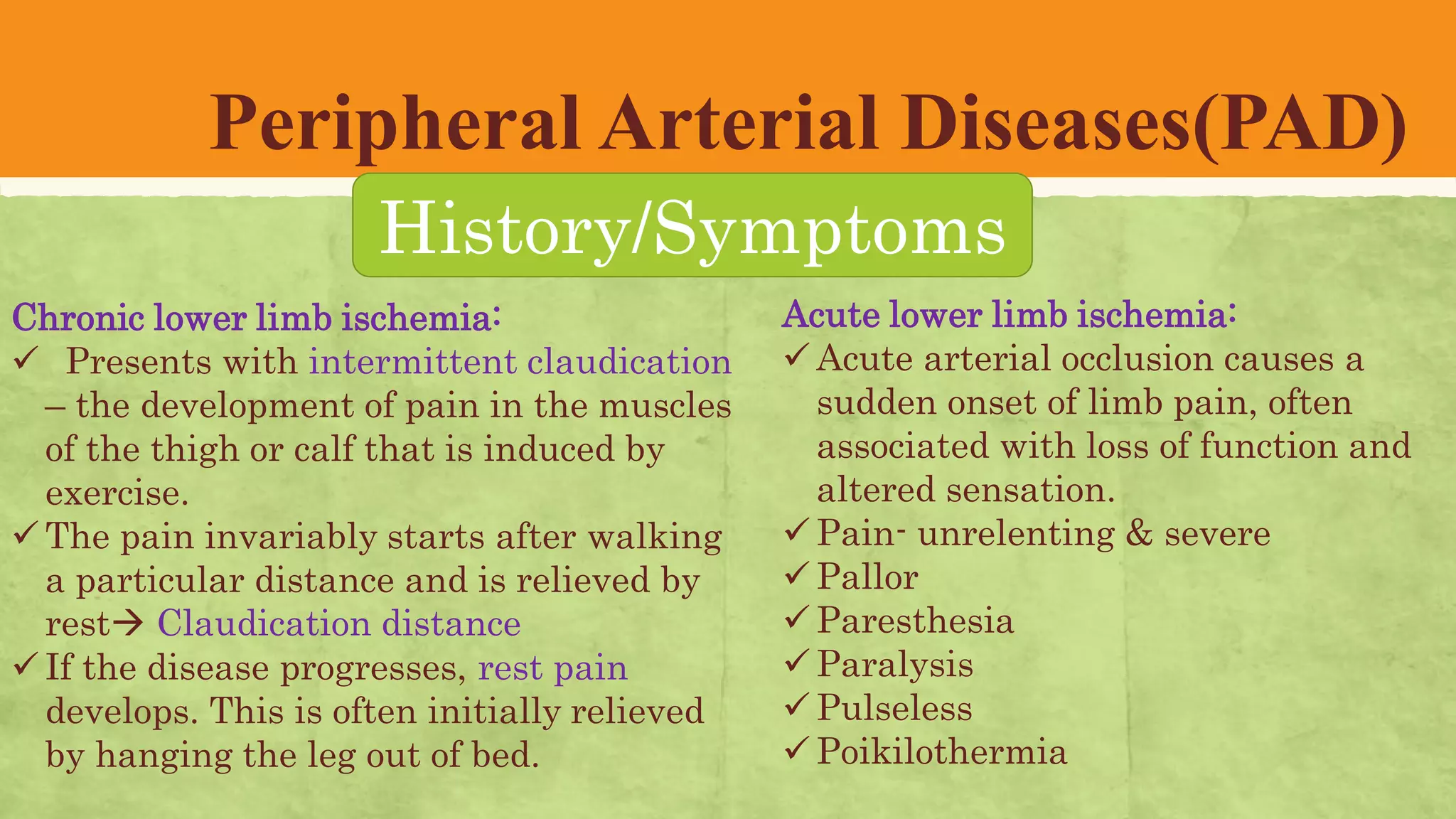
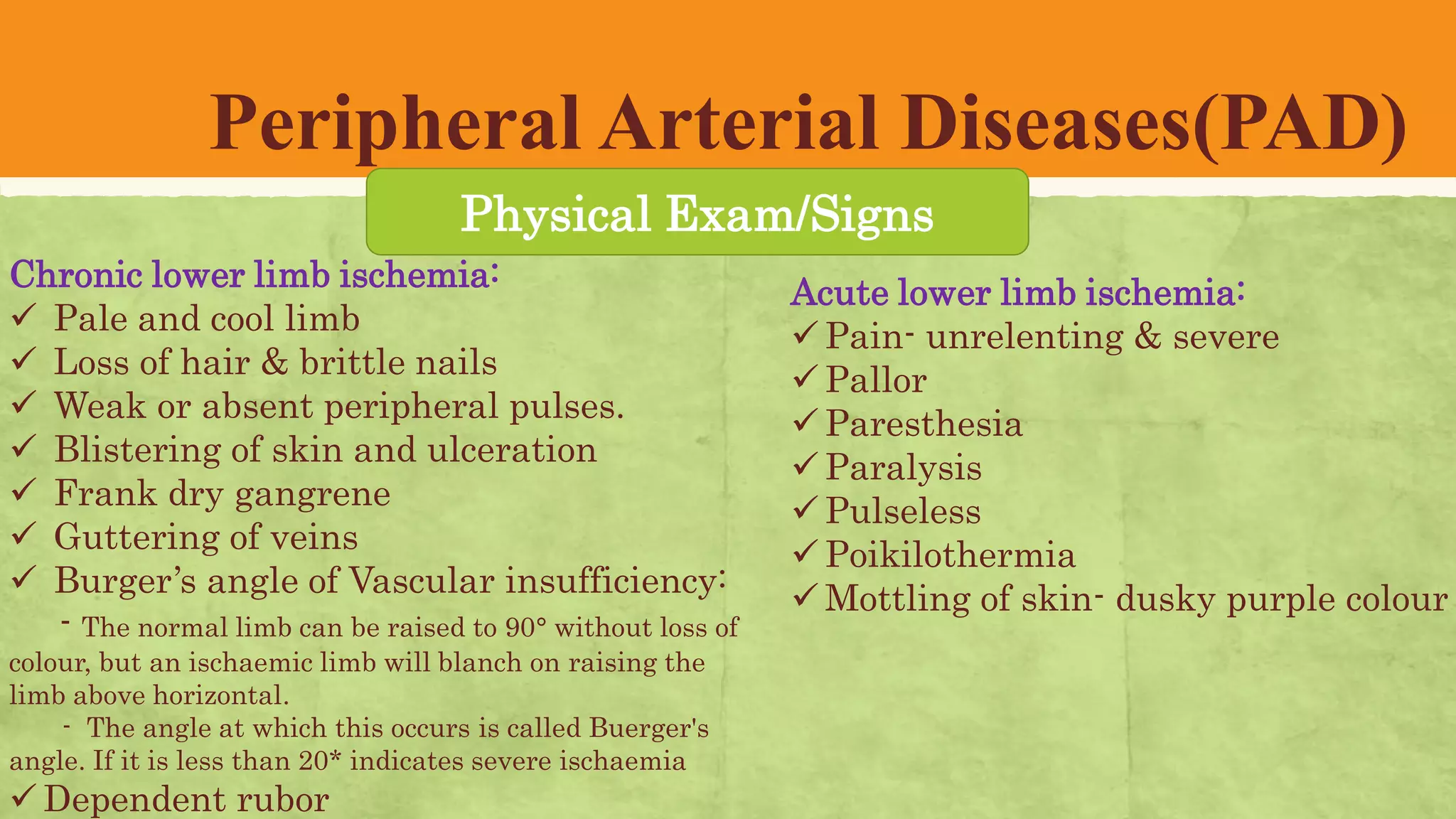
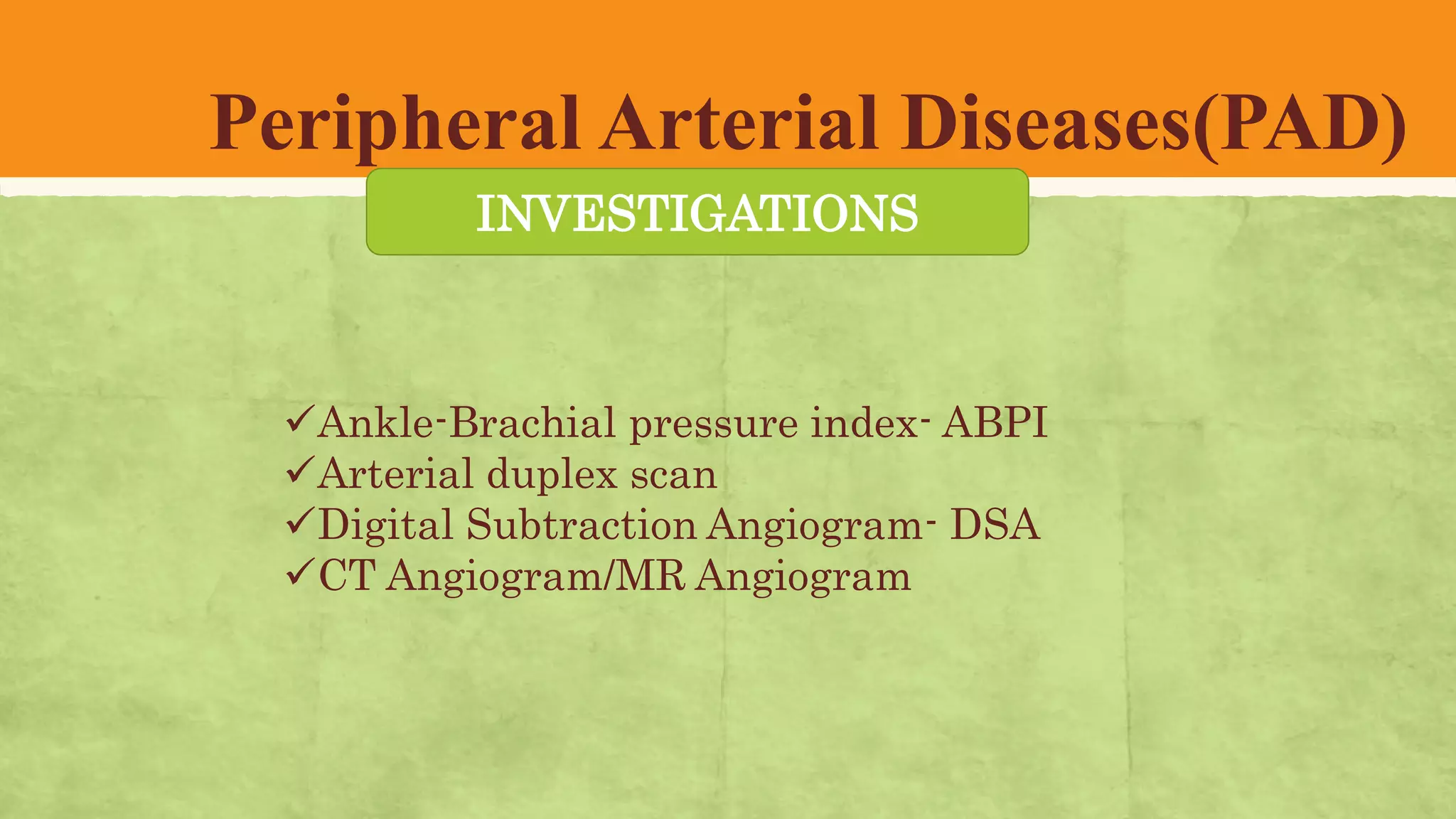




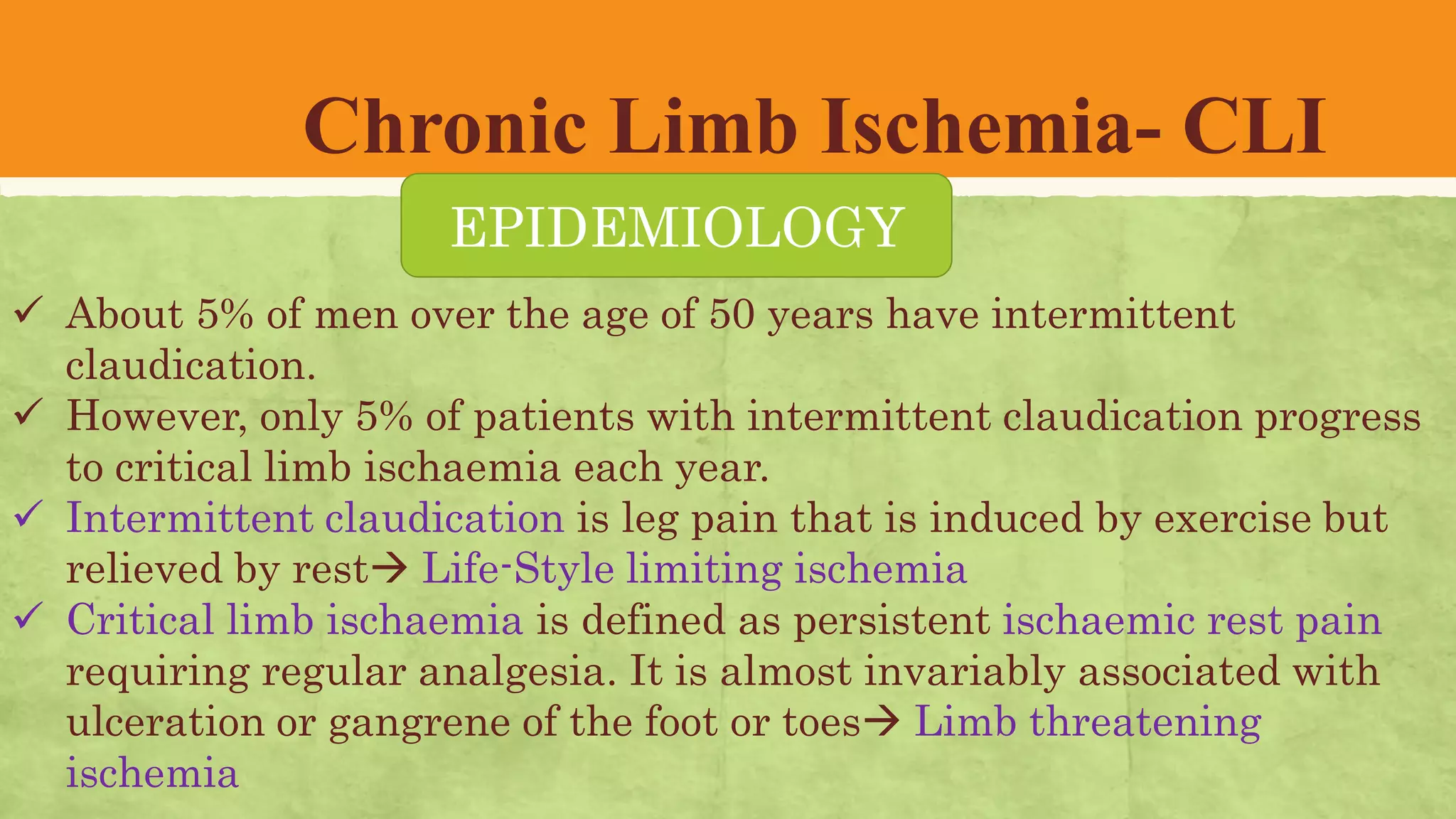












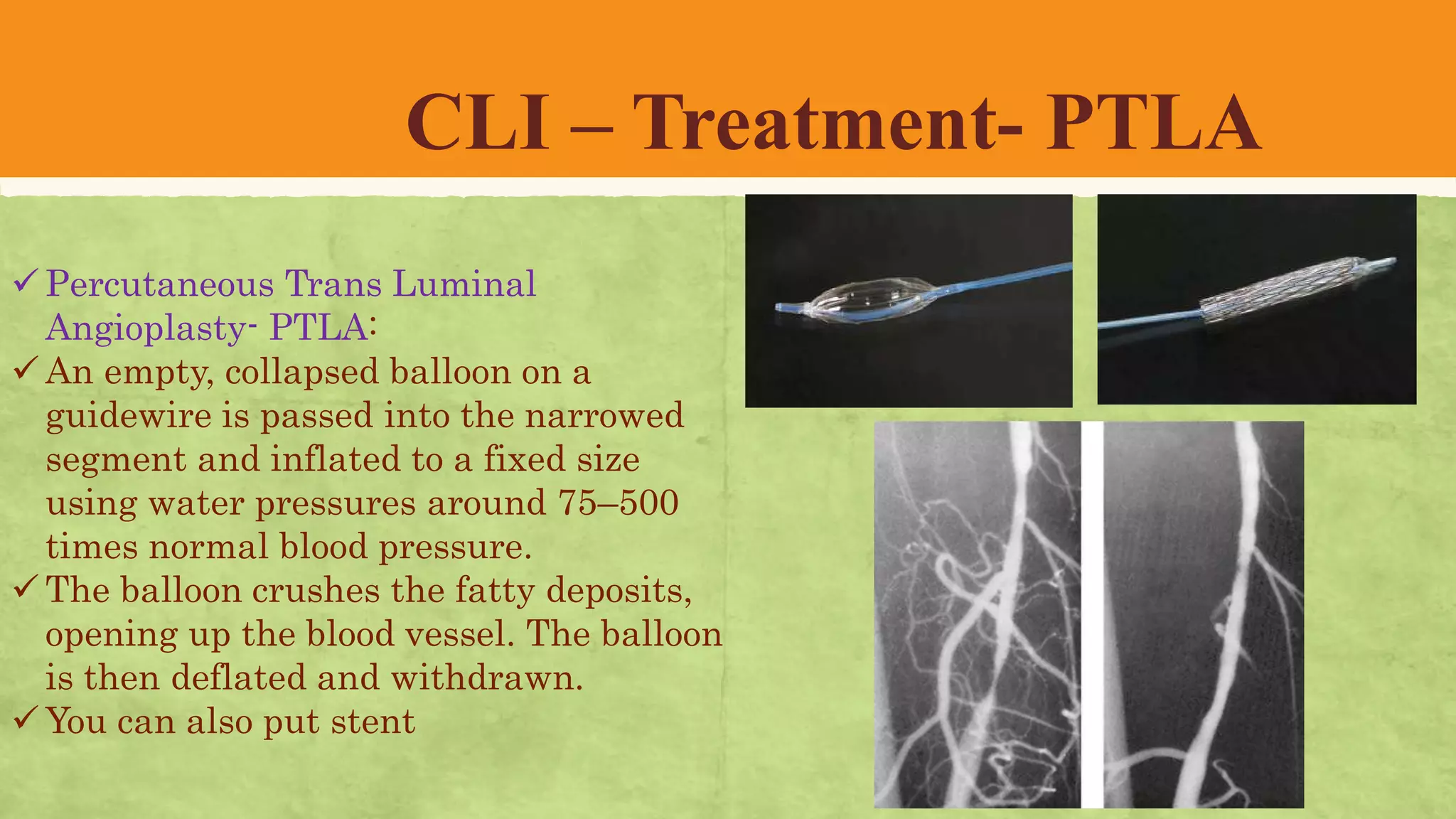









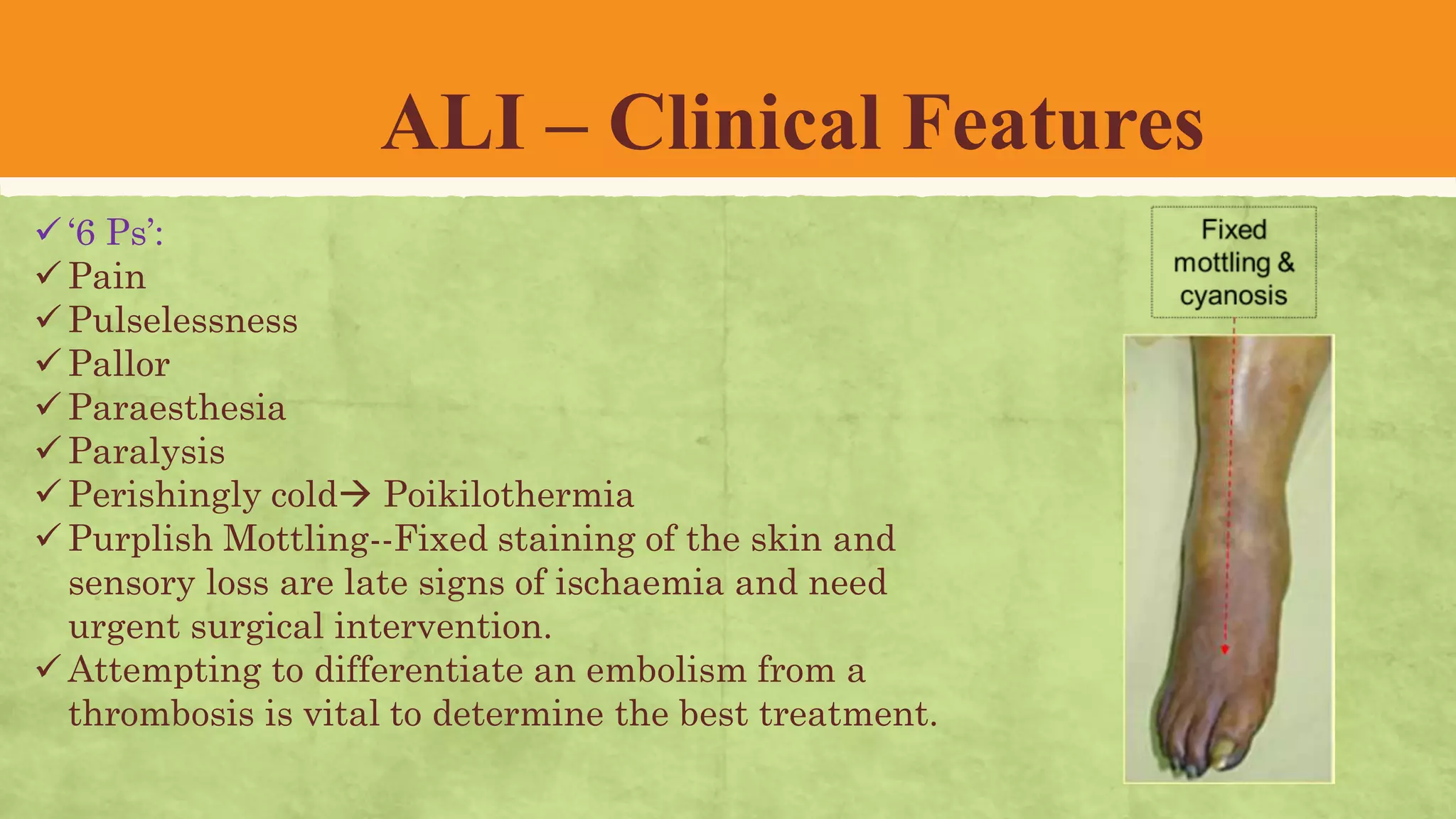



































The document provides a comprehensive overview of peripheral arterial diseases (PAD), their classifications, symptoms, pathophysiology, and treatment options. It focuses on both acute and chronic forms of limb ischemia, detailing clinical features, diagnostic investigations, and management strategies. Important aspects include acute limb ischemia's surgical emergency nature, chronic limb ischemia's lifestyle impacts, and various treatment methods such as revascularization and lifestyle modifications.












































![[QC-ed] AMSA_AMBOSS Lecutre - PAD.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/qc-edamsaambosslecutre-pad-230324194416-cd414909-thumbnail.jpg?width=640&height=640&fit=bounds)










































