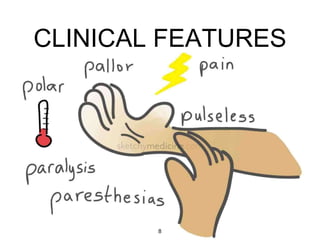
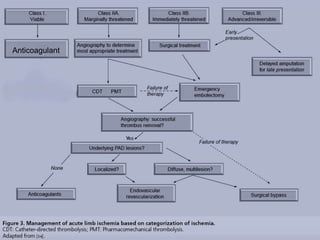
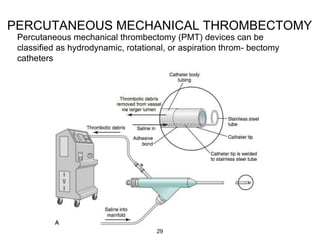
Acute limb ischemia is a sudden loss of blood flow to an extremity lasting less than two weeks that can lead to limb loss without prompt treatment. It requires rapid diagnosis through clinical examination, imaging tests like angiography, and treatment including anticoagulation, catheter-directed thrombolysis, percutaneous thrombectomy, or surgical revascularization to restore blood flow. Outcomes depend on how quickly circulation is reestablished, with higher rates of amputation or mortality associated with delays in treatment.













































![ESVS Guidelines ALI 2020 - MARGA compressed [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/esvsguidelinesali2020-margacompressedrepaired-221116034136-273c0e6d-thumbnail.jpg?width=640&height=640&fit=bounds)
















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

