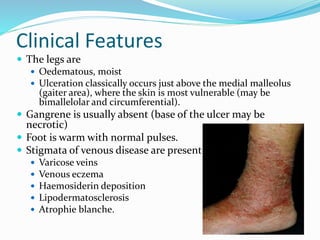
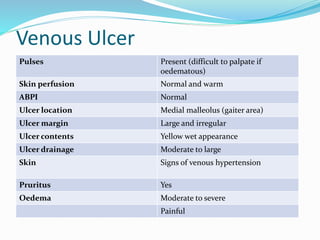
Venous ulcers account for nearly 80% of lower extremity ulcers and are caused by venous hypertension and reflux which damages the veins and capillaries. Risk factors include advancing age, family history, prolonged standing, obesity, smoking, and prior venous thrombosis. Conservative management involves compression therapy, elevation, exercise, and dressings. For severe or non-healing ulcers, surgical options like vein stripping or valvuloplasty may be used to correct venous reflux and lower pressure. Skin grafting can then promote wound closure.