- Peripheral vascular disease (PVD) refers to disorders affecting arteries, veins and lymphatics outside the heart and brain. More commonly it affects the arteries.
- PVD ranges from asymptomatic to critical limb ischemia with pain, ulcers or gangrene. Risk factors include smoking, diabetes, hypertension, hyperlipidemia, age and family history.
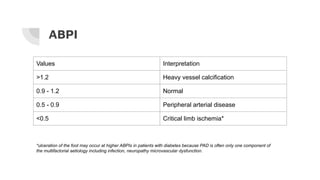
- Clinical features depend on location and severity, from intermittent claudication to critical limb ischemia. Investigations include ankle-brachial pressure index and imaging of arteries.
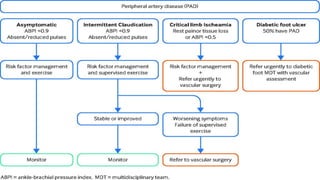
- Management involves risk factor modification, exercise/drugs for claudication, endovascular procedures, surgery like bypass, and amputation for critical cases. Compression therapy























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















