Downloaded 50 times







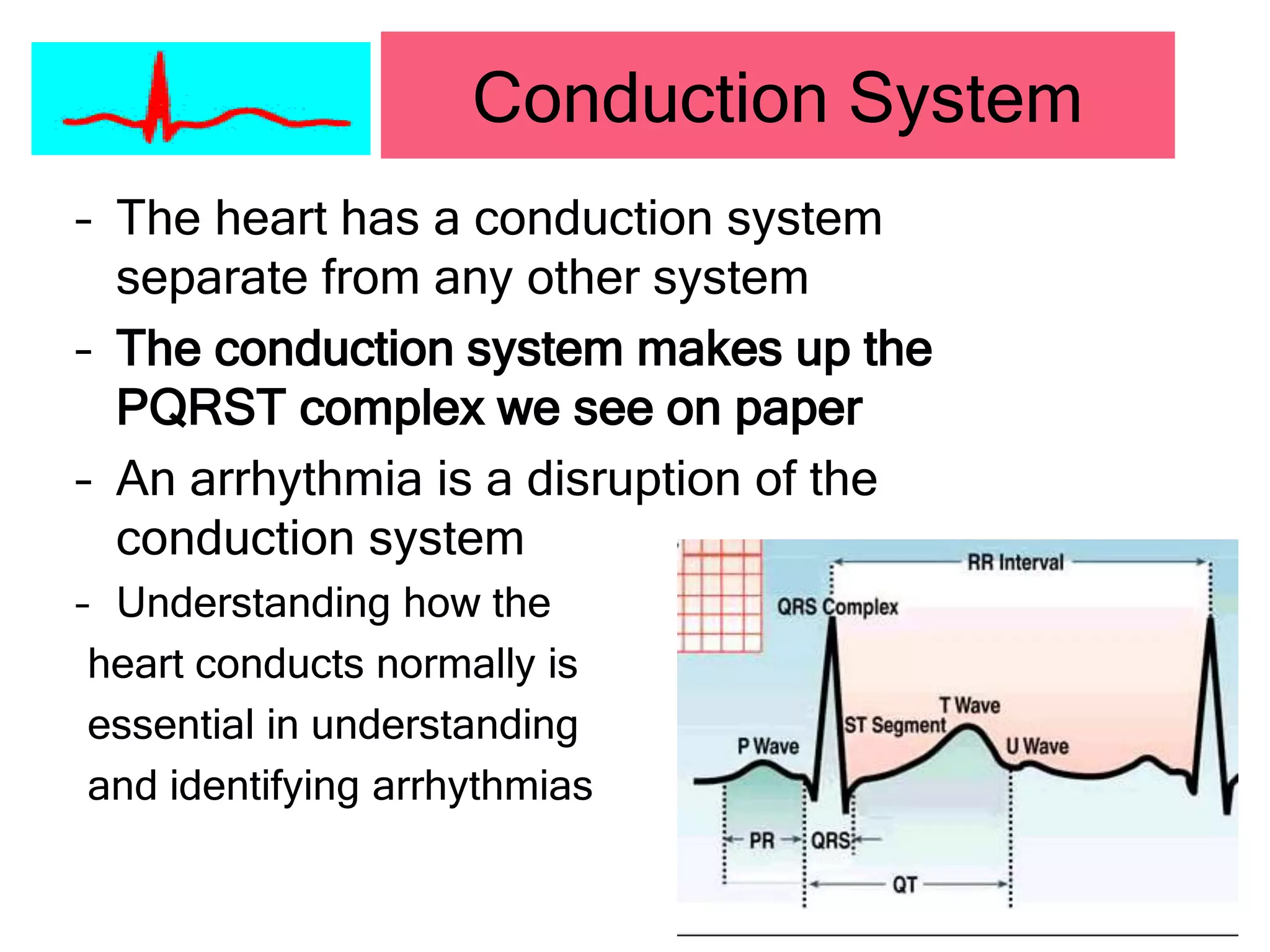

































































































This document provides information on cardiac arrhythmias, including: - The normal cardiac conduction system and blood flow through the heart. - Definitions and characteristics of various normal and abnormal sinus rhythms, atrial rhythms, junctional rhythms, and ventricular rhythms based on heart rate, rhythm, P wave presence and morphology, PR interval, and QRS width. - Key arrhythmias summarized include normal sinus rhythm, sinus bradycardia, sinus tachycardia, premature atrial contractions, atrial fibrillation, atrial flutter, premature junctional contractions, junctional tachycardia, premature ventricular contractions, ventricular tachycardia, and ventricular flutter.