Downloaded 1,326 times













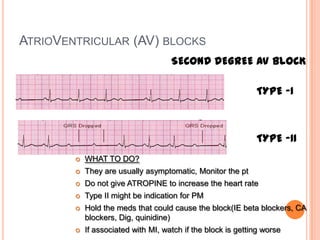



This document discusses cardiac arrhythmias and the cardiac conduction system. It describes the sinoatrial node, atrioventricular node, and Purkinje fibers, which make up the cardiac conduction system. Causes of arrhythmias include enhanced automaticity, triggered activity, and re-entry. Various arrhythmias are described including sinus bradycardia, premature atrial contractions, atrial fibrillation, premature ventricular contractions, ventricular tachycardia, and different types of atrioventricular block. The electrocardiogram is discussed as a tool to evaluate heart rate, intervals, waves, and diagnose arrhythmias.




































![Dysrhythmia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysrhythmiaautosaved-230617180733-e317f7a6-thumbnail.jpg?width=640&height=640&fit=bounds)






























