

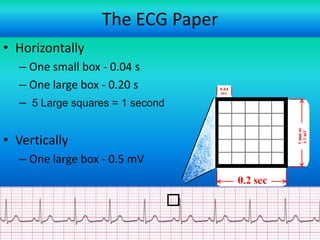
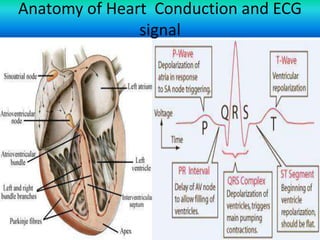
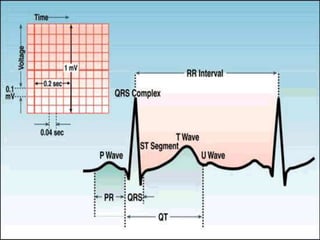
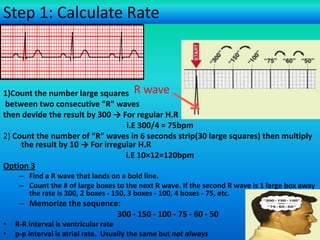
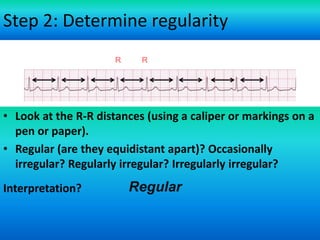
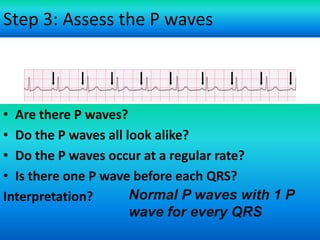
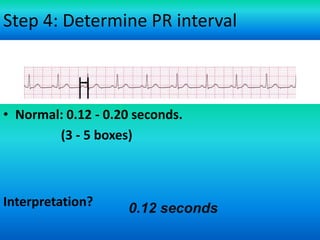
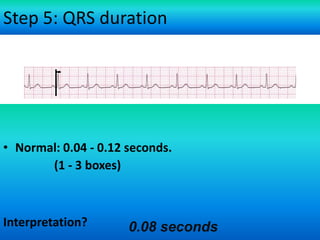
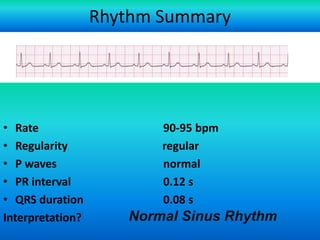
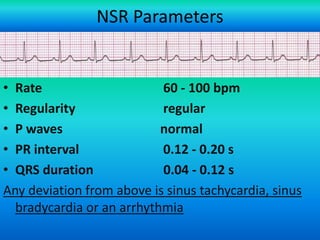
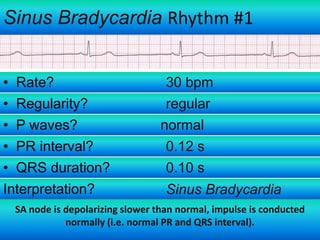
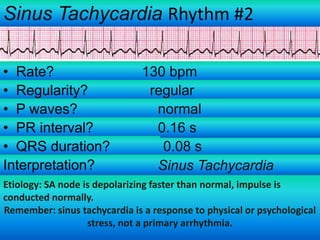
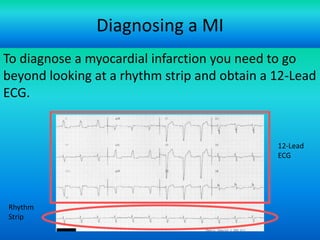


An ECG provides a representation of the heart's electrical activity during each cardiac cycle. It displays distinct waveforms that can provide insight into a patient's cardiac pathophysiology. The ECG paper displays time and voltage measurements to analyze rate, regularity, P waves, PR interval, and QRS duration in order to identify normal sinus rhythm or potential arrhythmias originating from problems in the sinus node, atria, AV node, or ventricles. Arrhythmias can cause the heart to beat too slowly, too quickly, or irregularly compared to normal sinus rhythm.




























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

