Downloaded 539 times
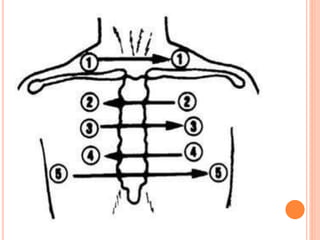
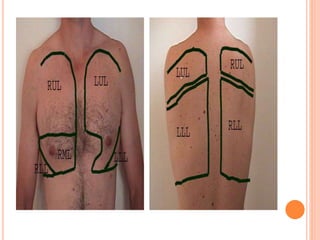
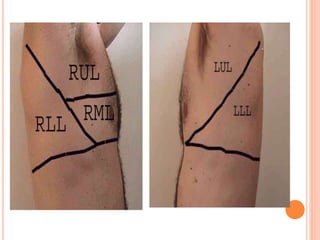
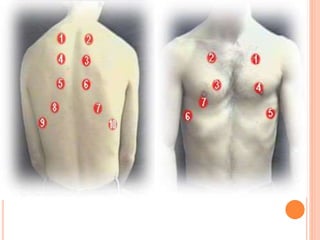
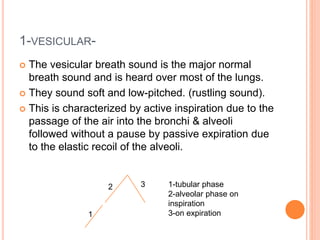


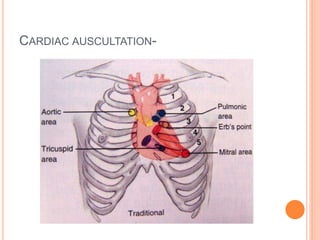
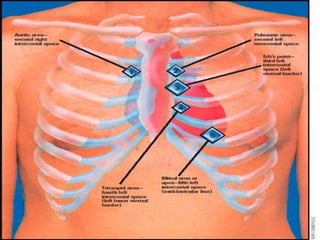

This document provides information on auscultating breath sounds and other body sounds. It describes how to properly auscultate breath sounds by placing the stethoscope on landmarks of the chest wall. Normal breath sounds are described as well as adventitious sounds such as crackles, wheezes, and rhonchi. The causes and characteristics of different breath sound types are explained. Proper cardiac auscultation is also briefly mentioned.






















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)












