Downloaded 92 times
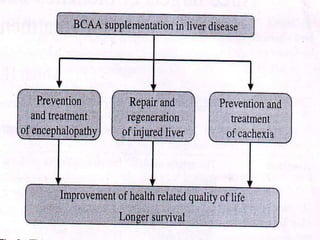
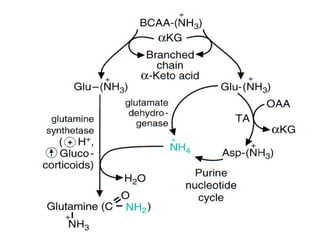
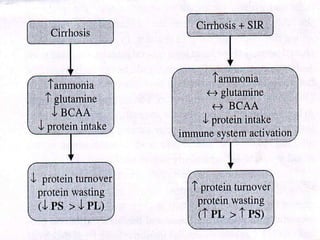

BCAA supplementation has three potential benefits for patients with liver disease: 1) It may help treat hepatic encephalopathy by promoting ammonia detoxification and reducing amino acid imbalances. 2) It may support liver regeneration through stimulating protein synthesis and secretion of growth factors. 3) It may help treat hepatic cachexia by stimulating protein synthesis and inhibiting proteolysis. The document discusses the mechanisms and evidence for these proposed benefits of BCAA supplementation for different types of liver injury and disease.