





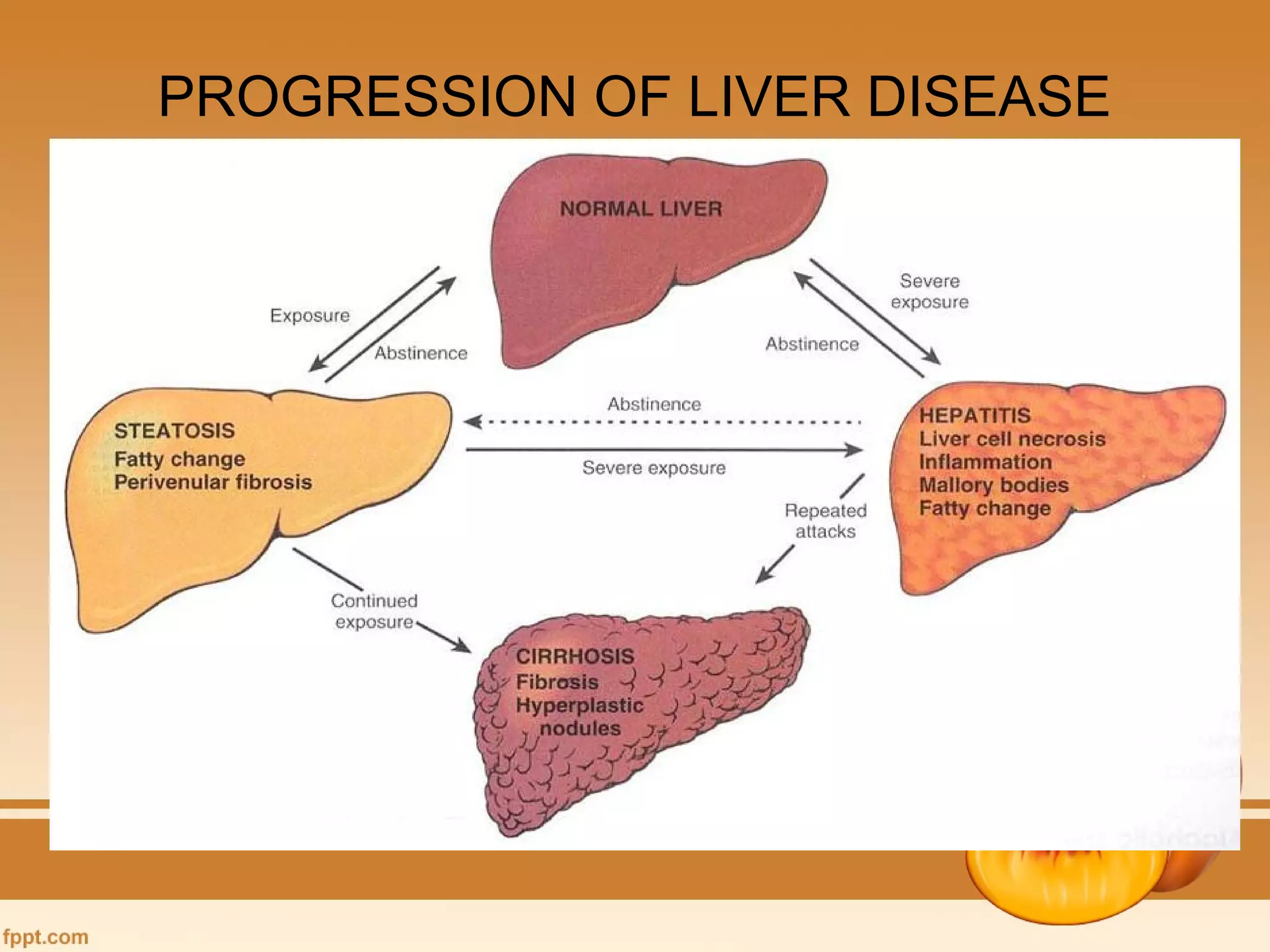


















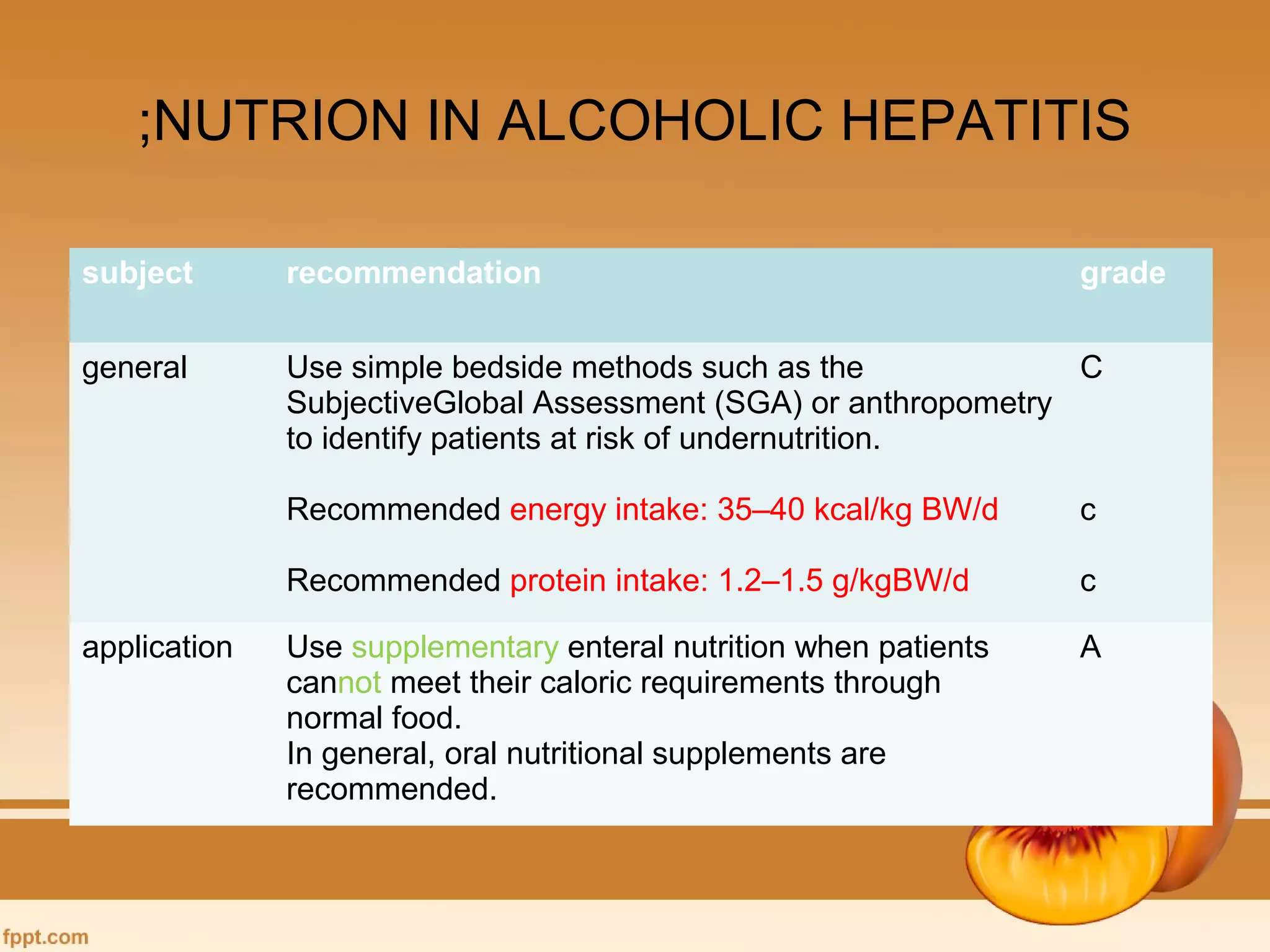


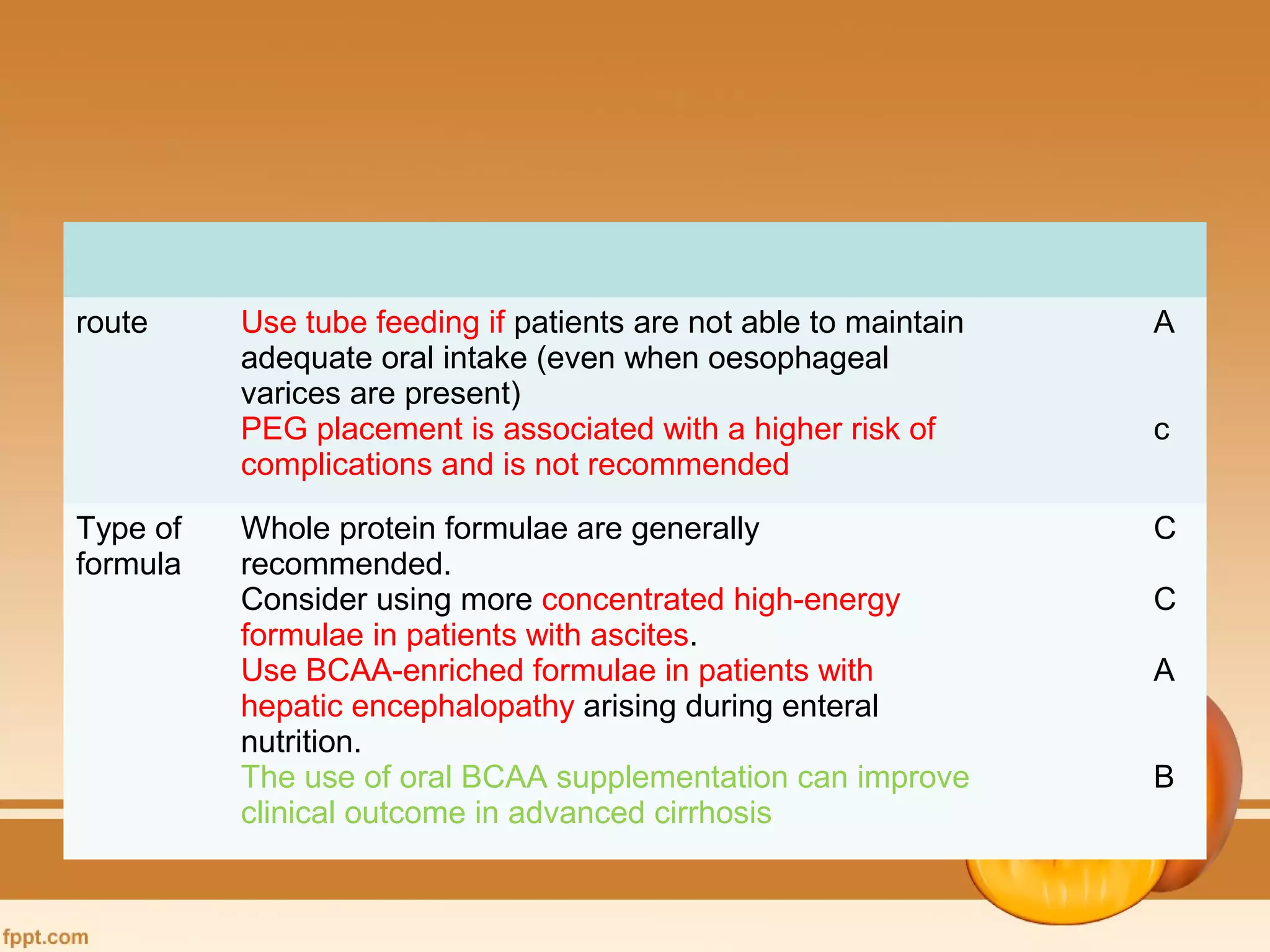














The document discusses liver disease and nutrition. It begins by reviewing the functions of the liver and various liver diseases. It then discusses nutritional features of end-stage liver disease and nutritional assessment and management guidelines. Specific topics covered include neurological symptoms associated with liver disease, nutritional assessment tools for patients with end-stage liver disease, daily energy expenditure calculation methods, progression of liver disease, and ESPEN guidelines on enteral and parenteral nutrition for various liver diseases.














































































