Downloaded 31 times










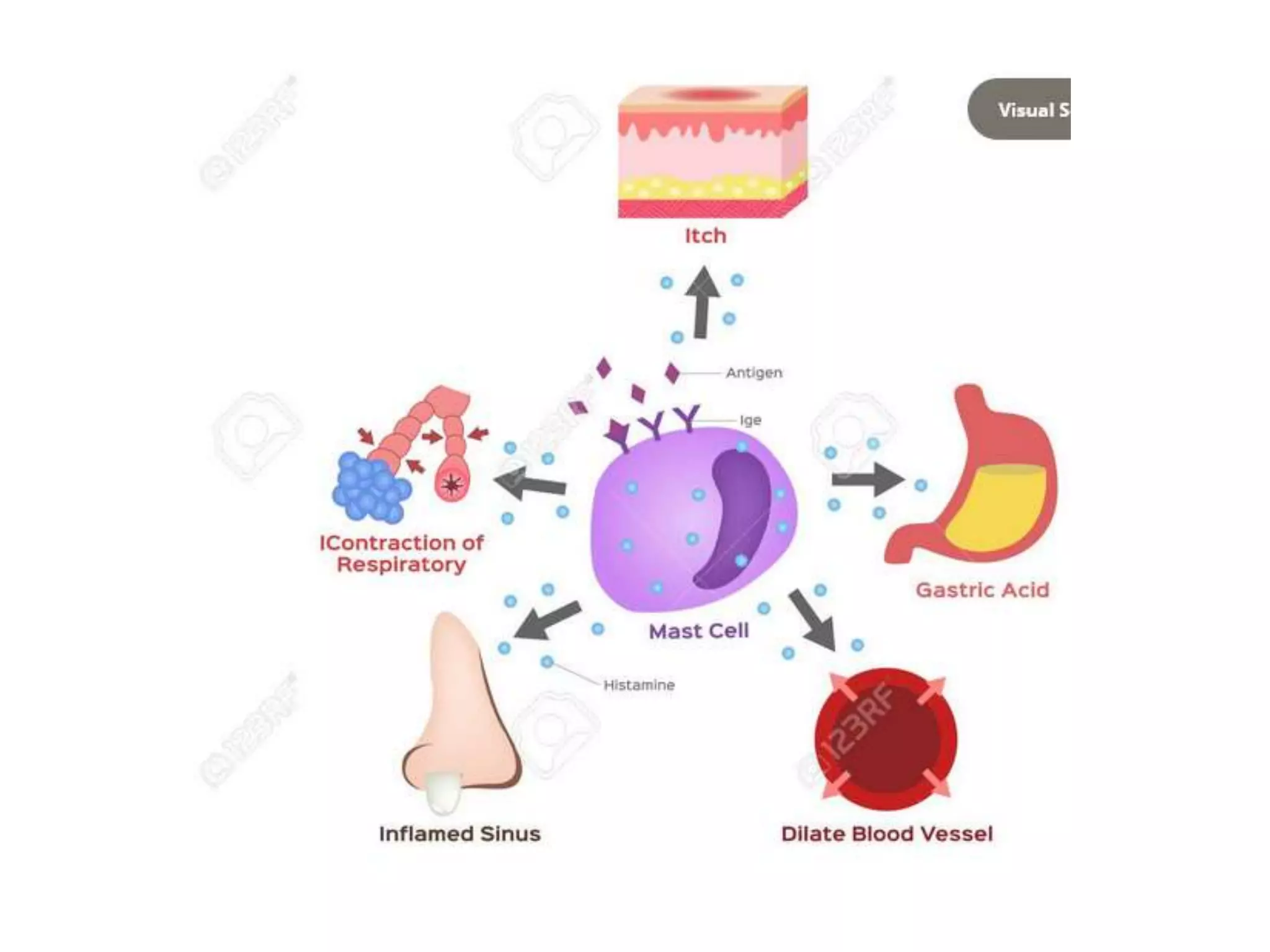

























































The document discusses autacoids, which are local biological substances produced by various body cells with intense biological activity, contrasting them with traditional hormones. It covers different types of autacoids, their functions, and role in pathophysiology, notably detailing histamine and serotonin as key examples. Additionally, it explains the pharmacological implications of antihistamines and lipid-derived autacoids such as prostaglandins and leukotrienes in treating various conditions, including allergies and inflammation.















































![lecture-4 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture-4autosaved-230730161044-605918a6-thumbnail.jpg?width=640&height=640&fit=bounds)







































