Downloaded 597 times

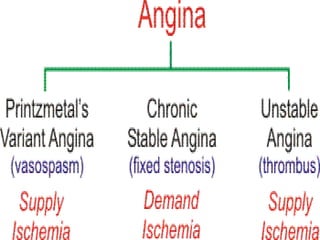
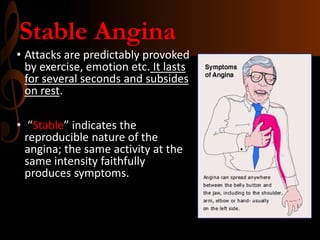

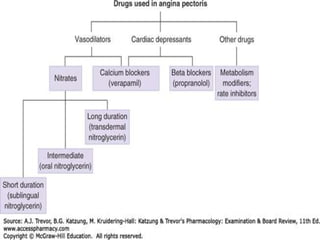


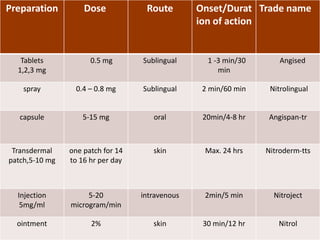

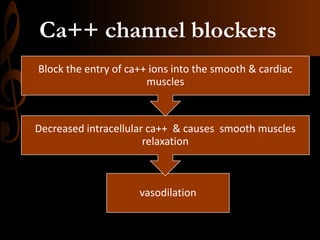

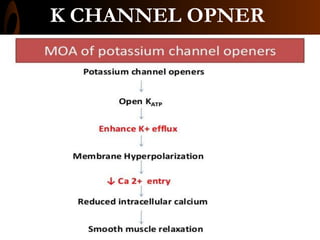


This document provides information about antianginal drugs used to treat angina pectoris. It discusses the three main types of angina and describes the mechanisms of action and uses of various antianginal drug classes including nitrates, beta-blockers, calcium channel blockers, and potassium channel openers. Specific drugs discussed include nitroglycerin, isosorbide mononitrate, atenolol, metoprolol, nifedipine, and nicorandil. Nursing responsibilities related to administration and patient education for these antianginal medications are also reviewed.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







