Downloaded 473 times
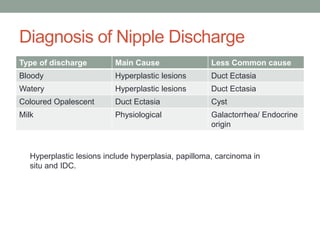
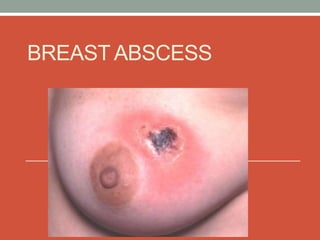
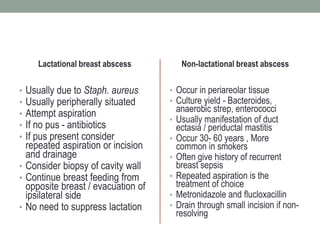
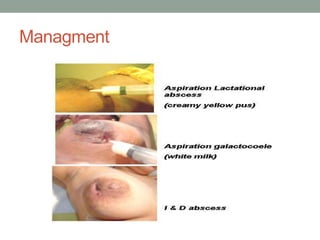

This document discusses several benign breast diseases including fibroadenoma, nipple discharge, and breast abscess. Fibroadenoma is the most common benign breast tumor, often appearing as a smooth, round, mobile mass. Nipple discharge can occur physiologically but bloody or persistent discharge warrants investigation to rule out hyperplasia or cancer. Breast abscesses commonly occur during lactation due to bacterial infection and are treated with aspiration or incision and drainage along with antibiotics.










































































