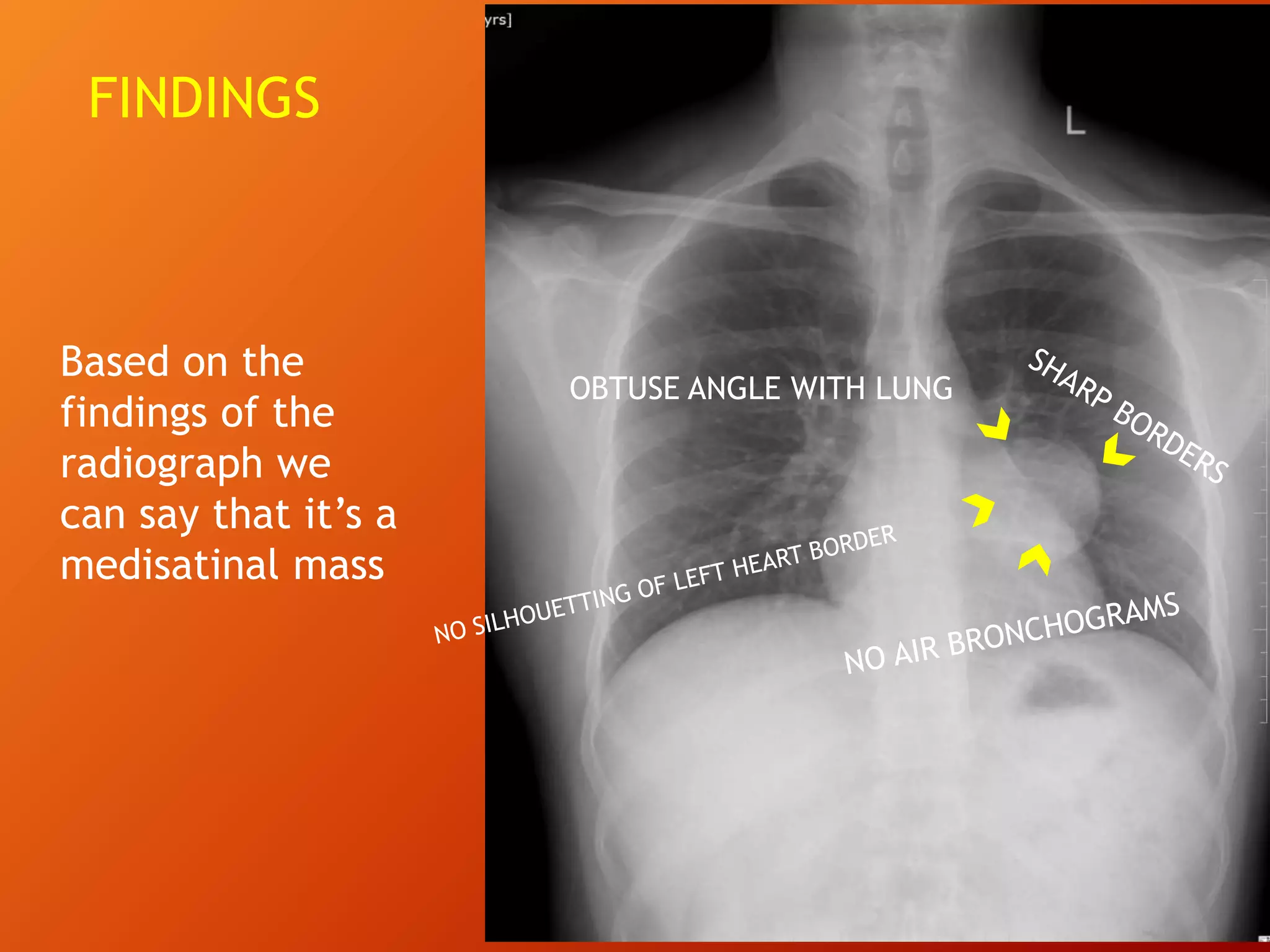
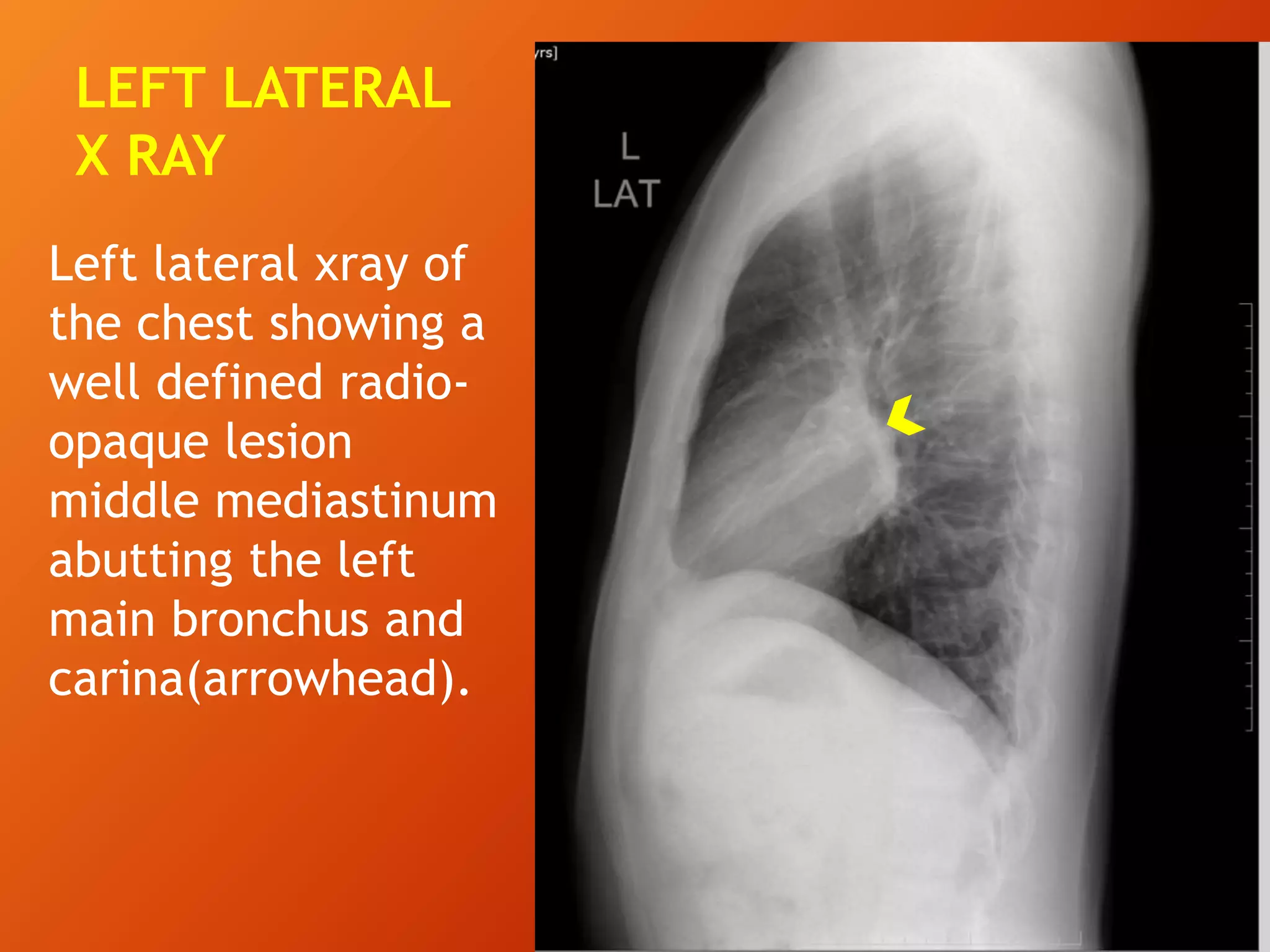
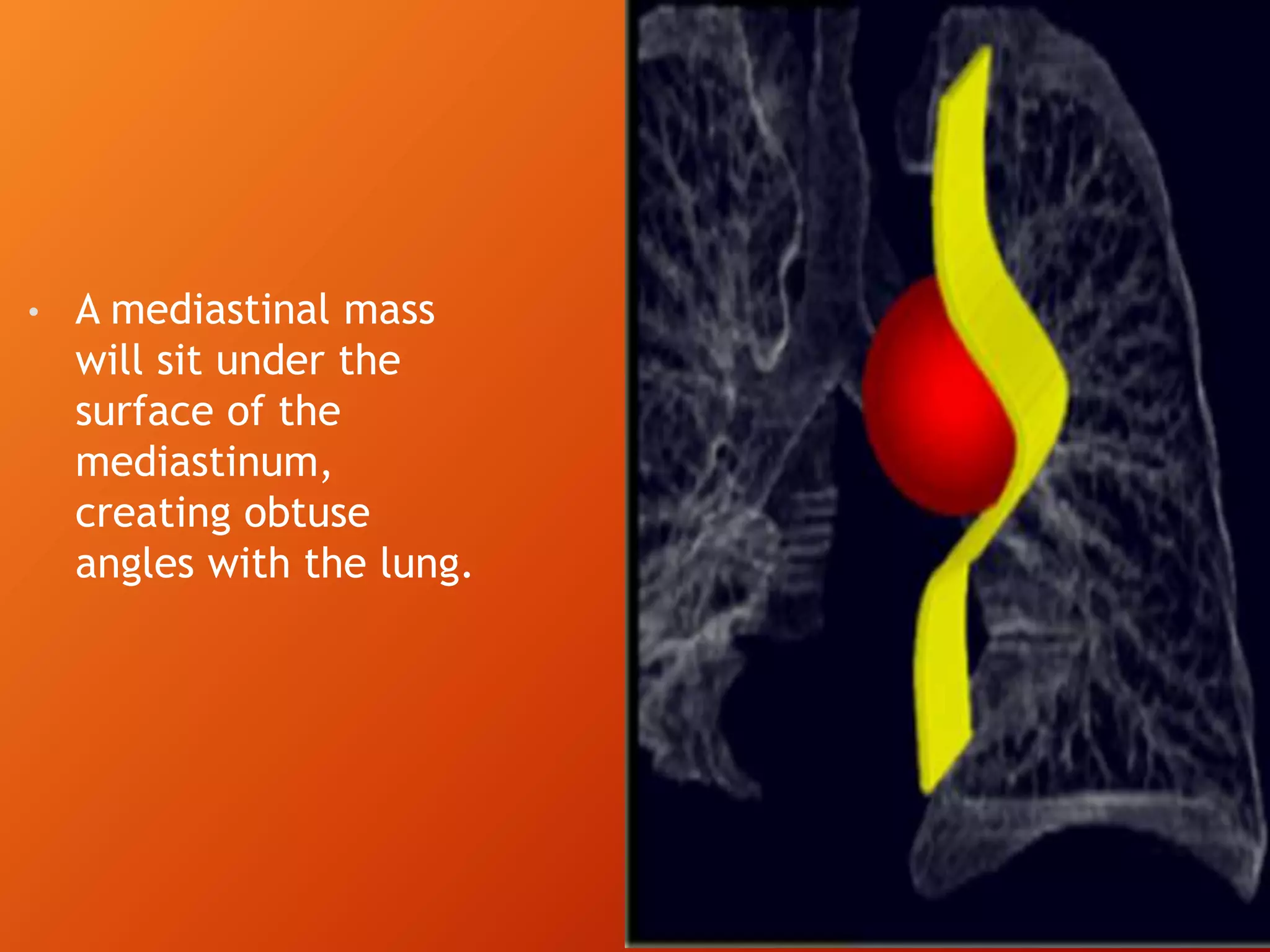
The document describes a case of a 27-year-old man presenting with chronic dry cough and referred for chest imaging. Chest x-ray revealed a well-defined round radio-opaque lesion in the left perihilar region. Further imaging found the mass to be arising from the left main bronchus in the middle mediastinum. Differential diagnoses included bronchogenic cysts and esophageal duplication cysts. Based on features of a sharply demarcated mass arising from the bronchus, the final diagnosis was determined to be a bronchogenic cyst, a congenital malformation of the bronchial tree.