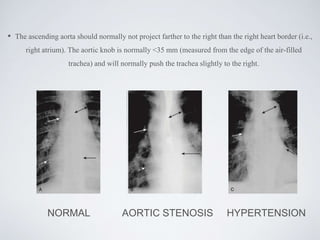
This document provides an introduction to chest radiography. It discusses the history of chest x-rays, the basic densities seen on x-rays, different views including PA, AP, lateral views, and how to evaluate technical adequacy. It also reviews normal pulmonary, pleural, and cardiac anatomy as seen on chest x-rays, and provides an overview of interpreting chest x-ray findings. The document is intended as an educational guide for radiology presenters and moderators.