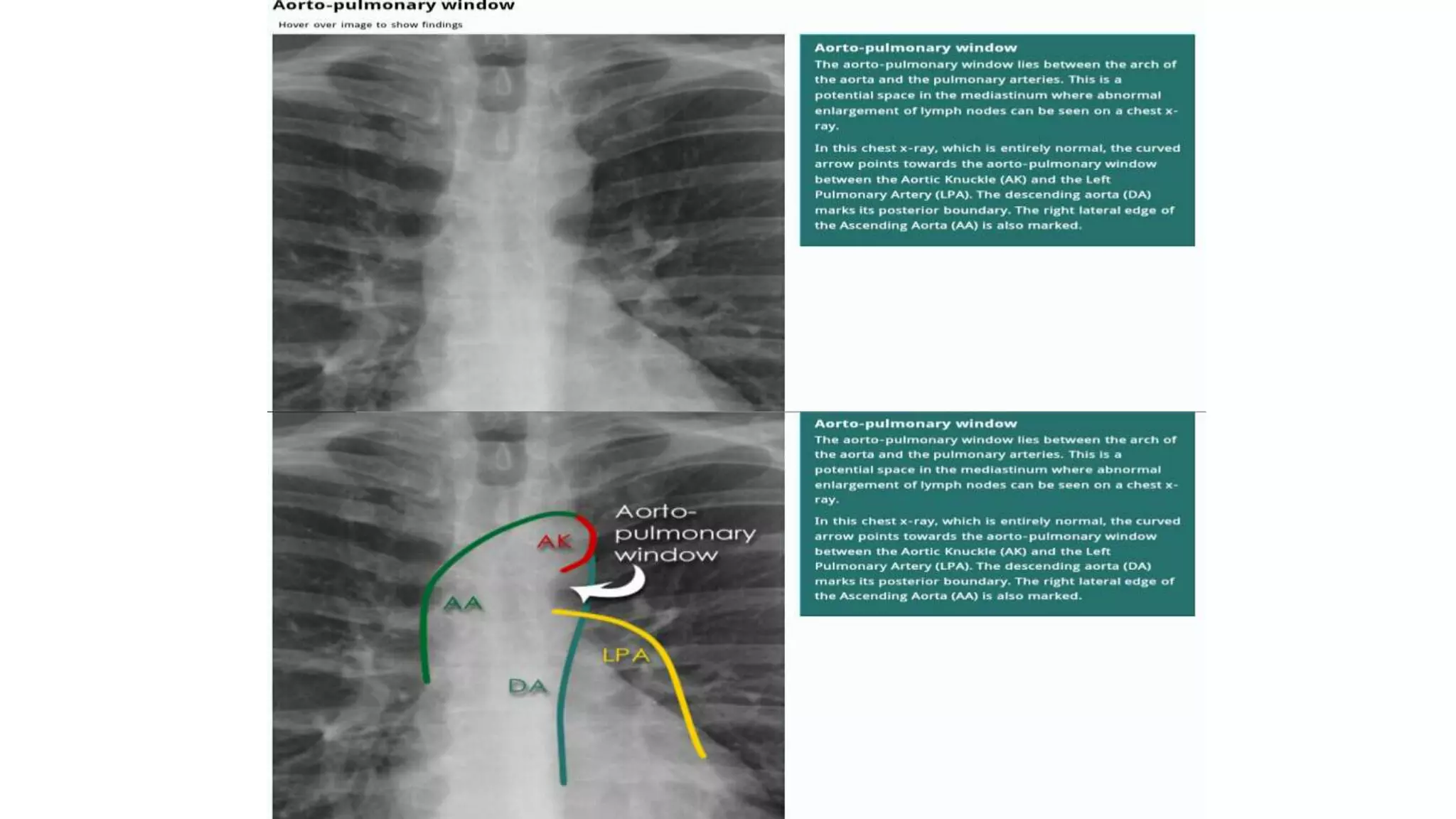
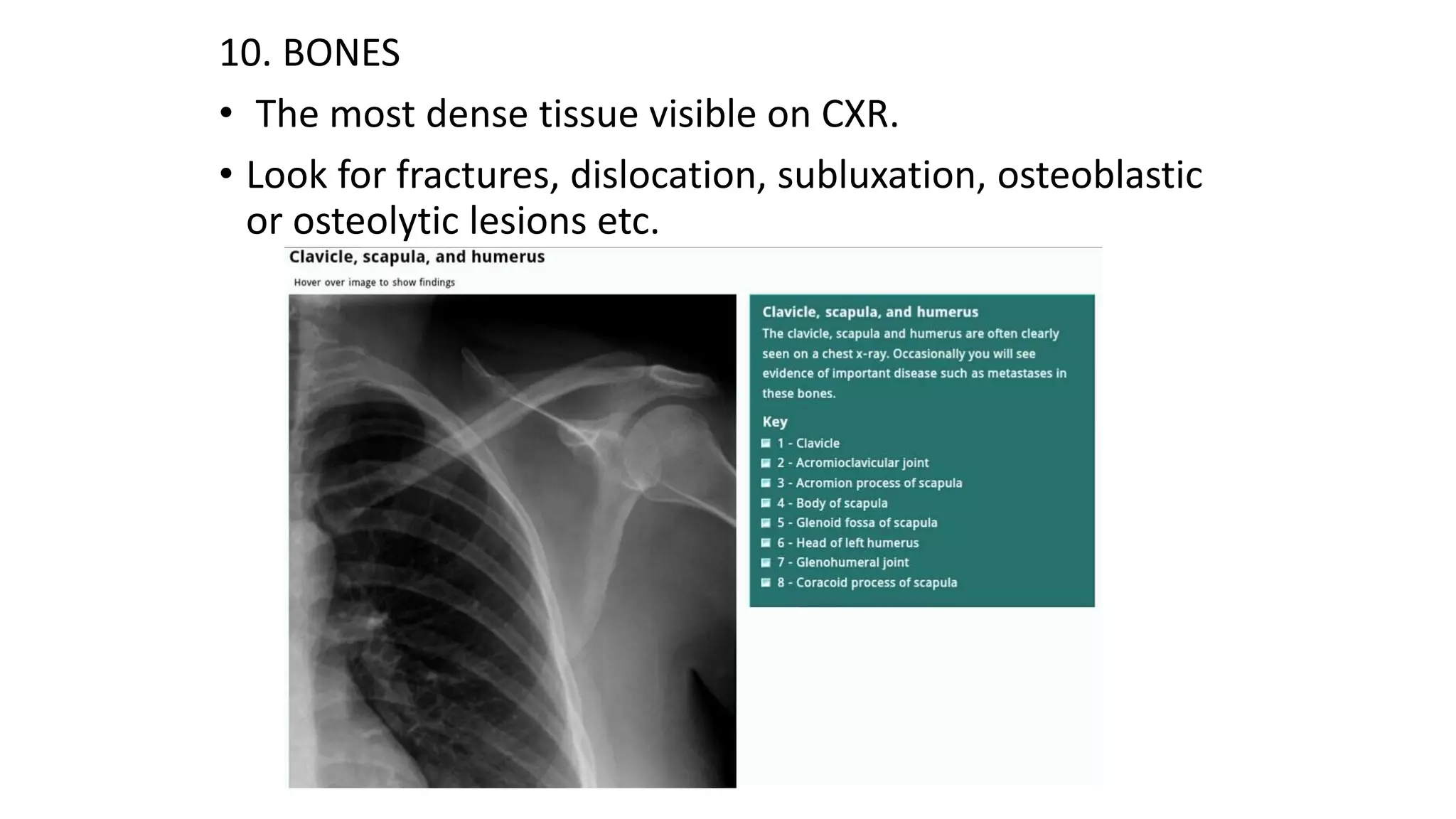
Chest X-rays provide important diagnostic information by visualizing the lungs, heart, bones and soft tissues. The document outlines key elements to evaluate on a chest X-ray including patient details, image quality, projection, inspiration, rotation, penetration and anatomy. Proper evaluation of these technical factors ensures accurate interpretation. Ten structures are identified: trachea, hilar structures, lungs, pleura, costophrenic angles, hemidiaphragms, heart, mediastinum, soft tissues and bones. Abnormalities should be described in detail and the most striking found first before checking the rest of the image.








































































![Radiological_diagnosis_of_TB_ECHO_MOH[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicaldiagnosisoftbechomoh1-240905083452-eb26e5f9-thumbnail.jpg?width=640&height=640&fit=bounds)























