Download to read offline





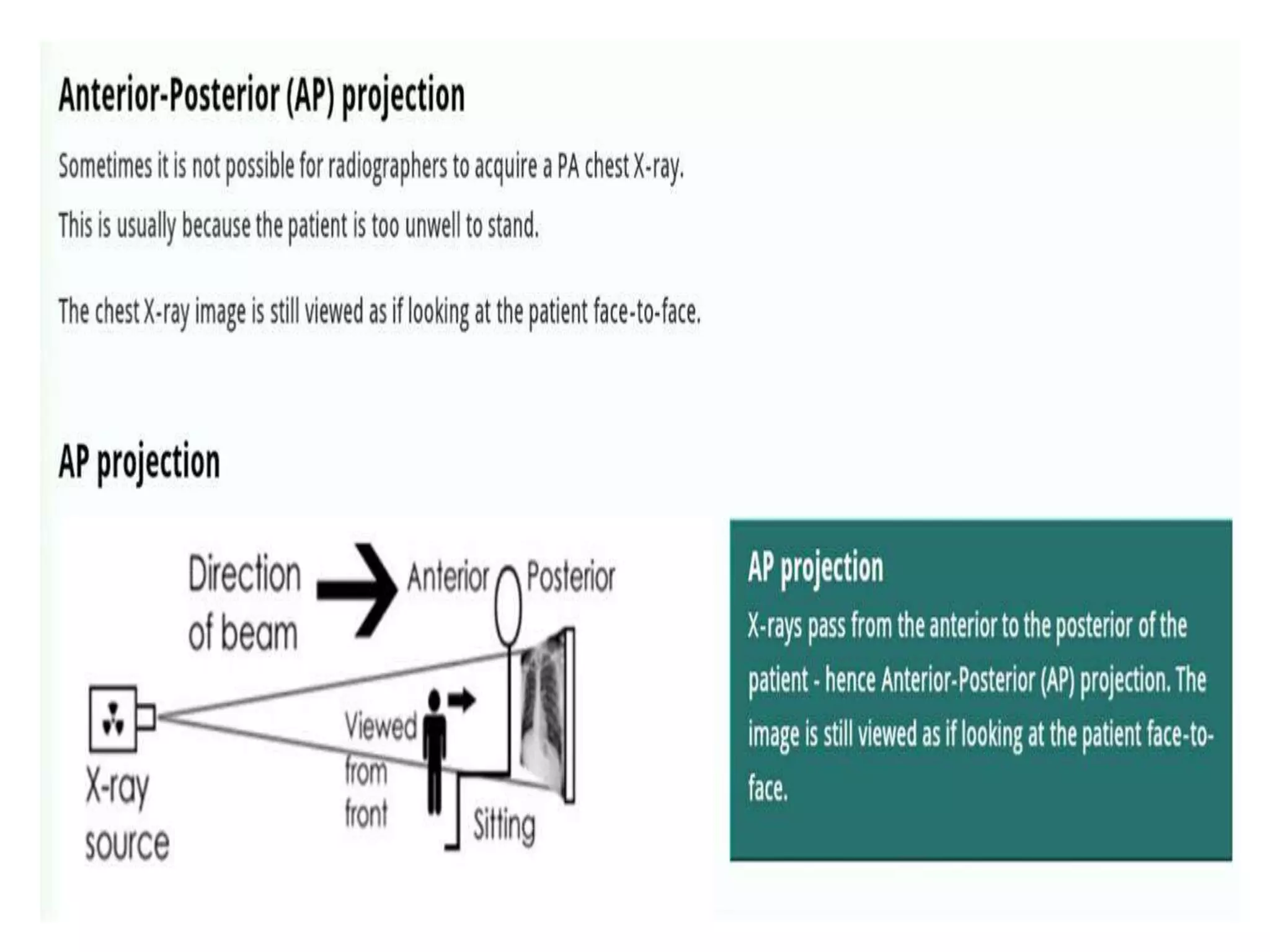







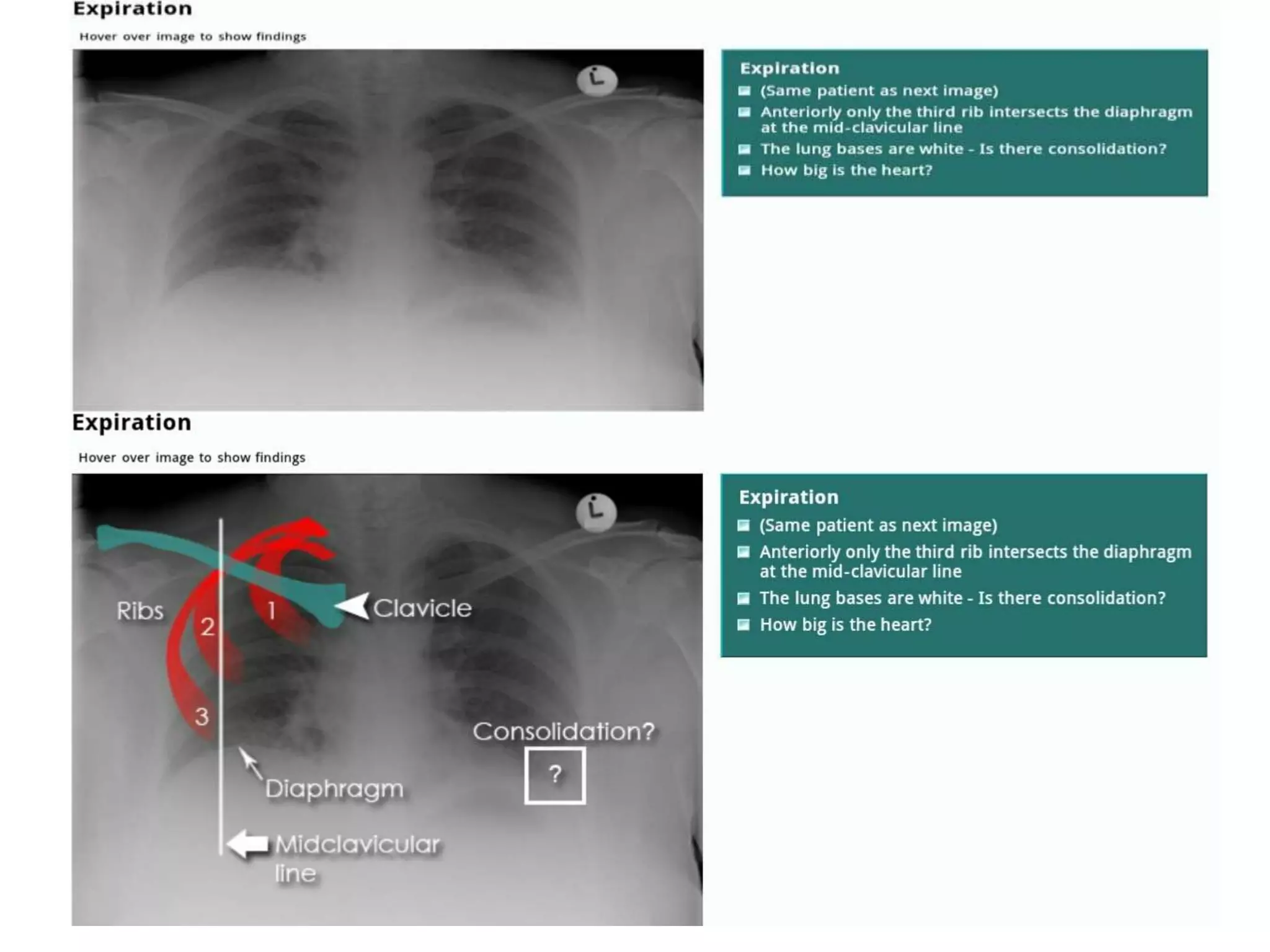


























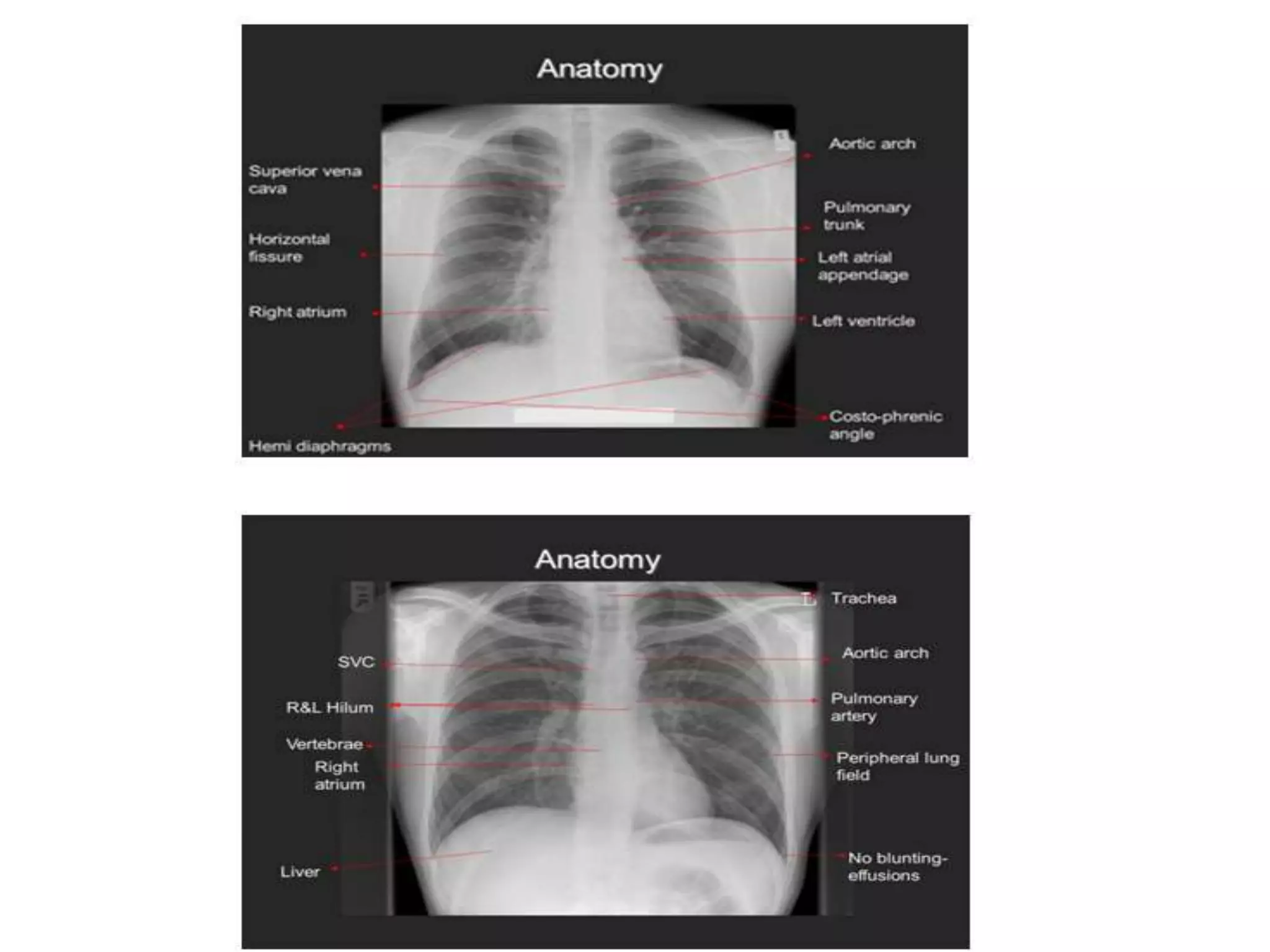














This document provides guidance on interpreting chest x-rays (CXRs). It discusses evaluating the quality, anatomy, and abnormalities visible on CXRs. Key points covered include checking for proper patient positioning, inspiration, and penetration. The anatomy discussed includes the lungs, heart, trachea, diaphragm, and bones. The document provides tips for systematically interpreting CXRs such as describing the most striking abnormality first before checking the rest of the image. The overall goal of interpretation is to be able to answer the clinical question.






































![Radiological_diagnosis_of_TB_ECHO_MOH[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicaldiagnosisoftbechomoh1-240905083452-eb26e5f9-thumbnail.jpg?width=640&height=640&fit=bounds)


























![Genetic Basis & Clinical Features of Achondroplasia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/geneticbasisclinicalfeaturesofachondroplasiaautosaved-240504095205-862c43d1-thumbnail.jpg?width=640&height=640&fit=bounds)





















