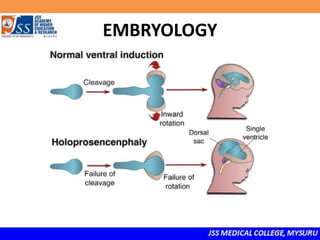
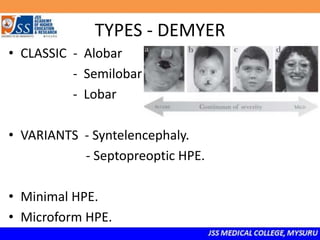
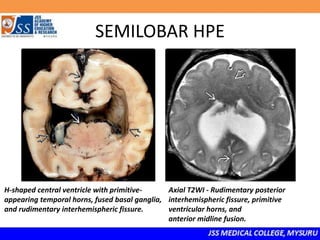
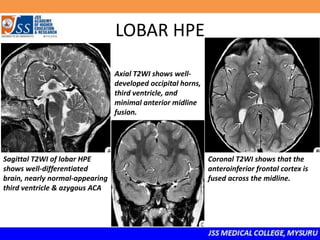
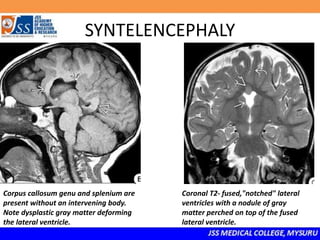
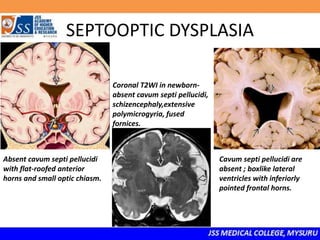
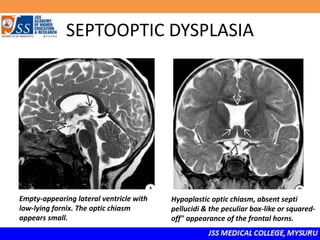
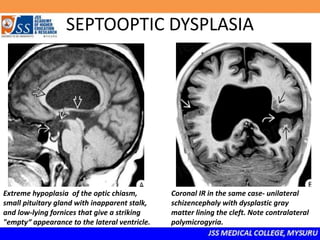
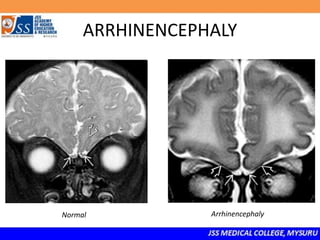
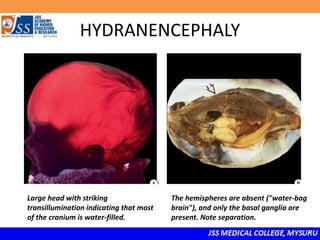
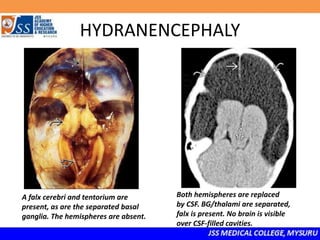
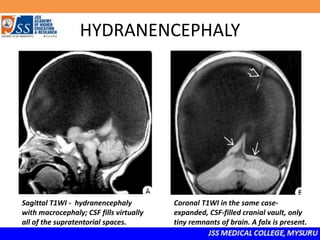
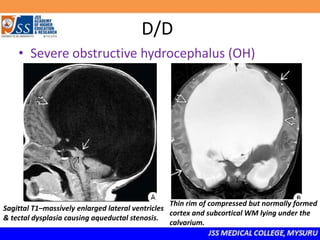
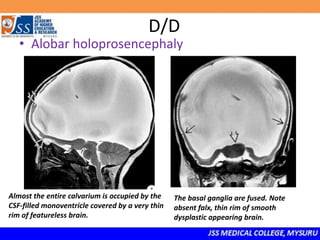
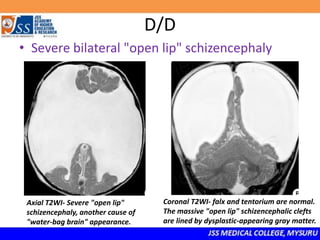
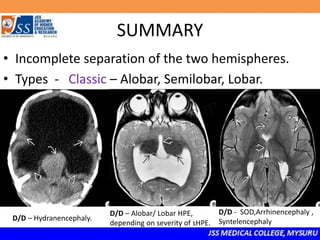
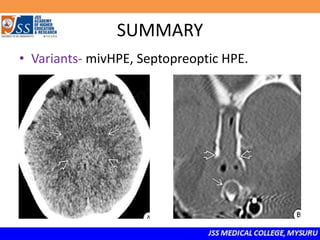
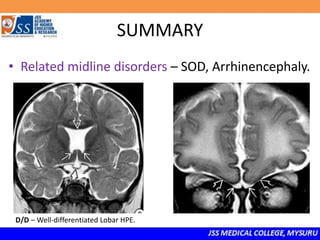
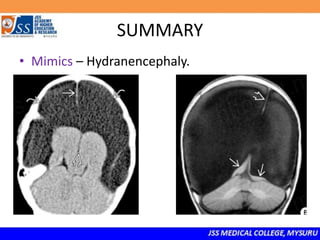
- Holoprosencephaly is a rare brain malformation caused by incomplete separation of the brain hemispheres. It can range from mild to severe forms depending on the degree of separation, and is classified as alobar, semilobar, or lobar. Related disorders include septo-optic dysplasia, syntelencephaly, and arhinencephaly. Hydranencephaly, where most of the brain is replaced by cerebrospinal fluid, is an important mimic. Prenatal diagnosis is possible as early as 6 weeks and involves looking for abnormal facial features and absence of the cavum septum pellucidum.













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



