Dr. Arohi Sharma's document summarizes the clinical presentation and assessment of ankylosing spondylitis (AS). Some key points:
- AS most commonly affects those from early 20s to 40s and is more common in males. Symptoms include chronic back pain improved by exercise.
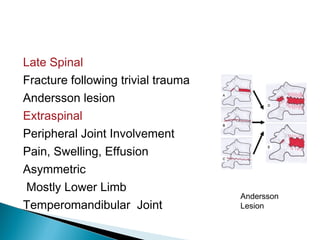
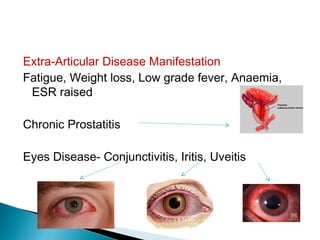
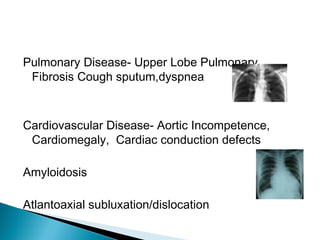
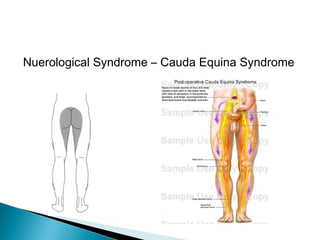
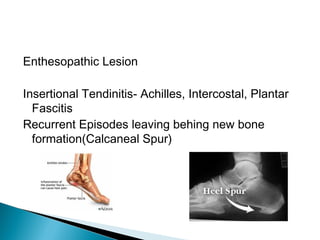
- Late stage AS can involve fractures from minor trauma or lesions. Extra-spinal manifestations may include peripheral joint involvement, eye/lung/heart issues, or neurological problems.
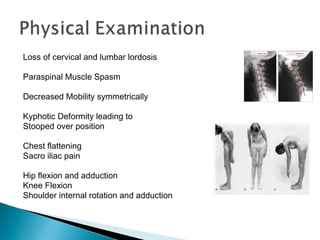
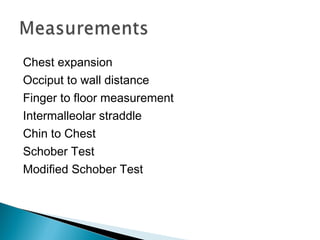
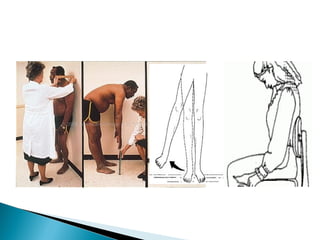
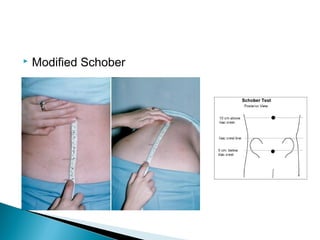
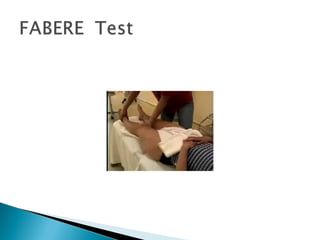
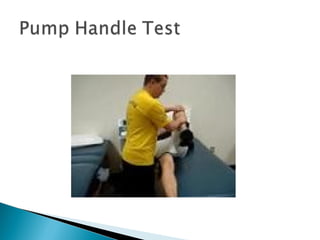
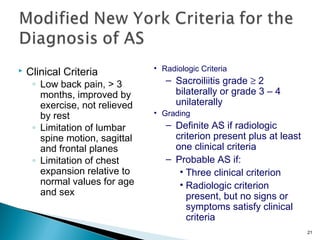
- Clinical assessments for AS include range of motion tests, chest expansion measurements, and sacroiliac imaging. Definite AS requires radiologic sacroiliitis plus one clinical criterion.
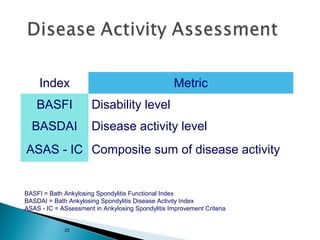
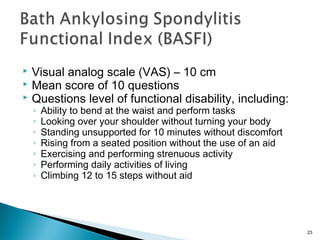
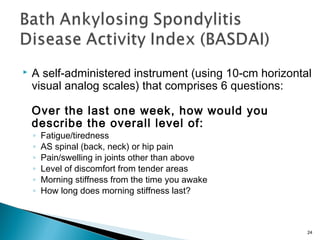
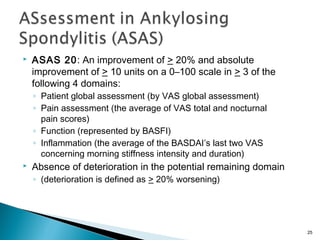
- Disease activity and functional