- Ankylosing spondylitis (AS) is a chronic inflammatory arthritis affecting the sacroiliac joints and spine that can lead to complete bony fusion. It has a strong association with the HLA-B27 gene.
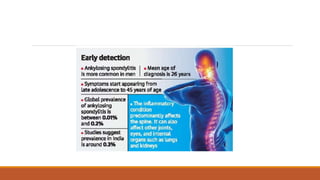
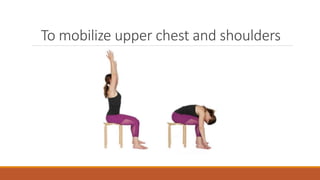
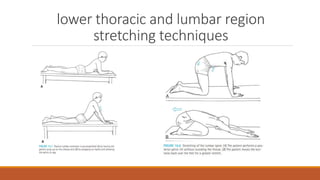
- Clinical features include morning stiffness and low back pain that improves with movement. The disease progresses to involve the entire spine and cause rigidity. Peripheral joints may also be affected.
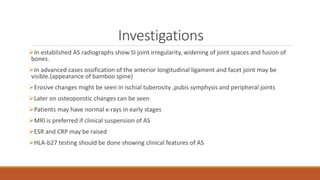
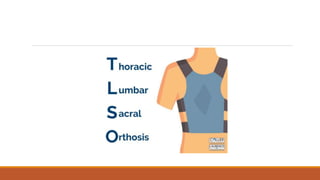
- Diagnosis is based on clinical features and confirmed with imaging showing sacroiliac joint changes or elevated inflammatory markers. There is no cure, but treatment focuses on exercises, medications, and lifestyle modifications to relieve symptoms and prevent deformities.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

