Downloaded 33 times
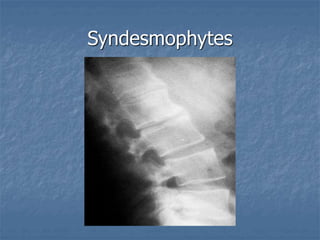

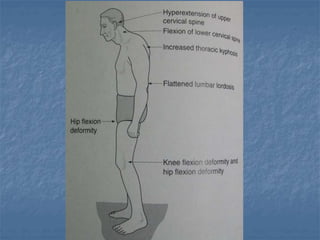
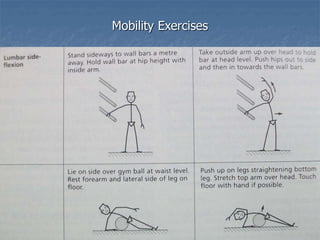
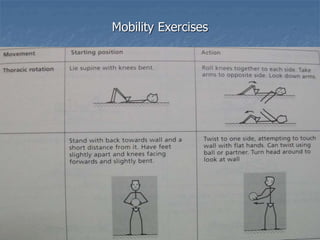
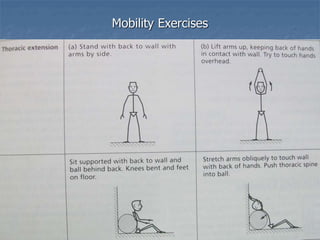
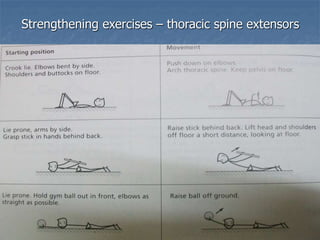
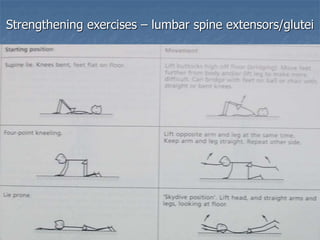
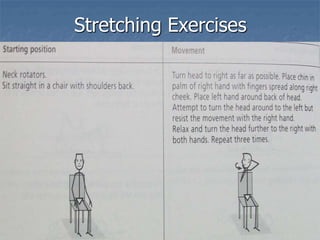
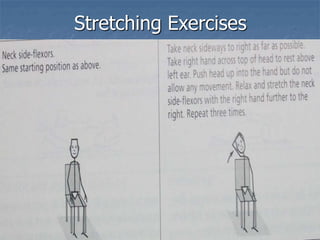
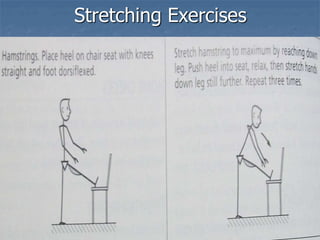
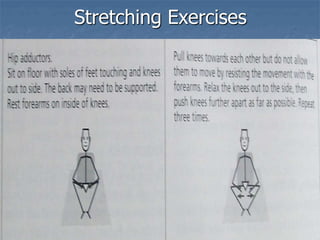
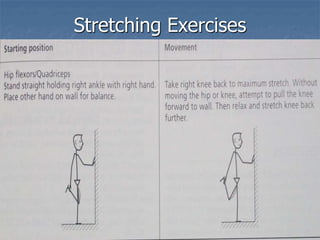
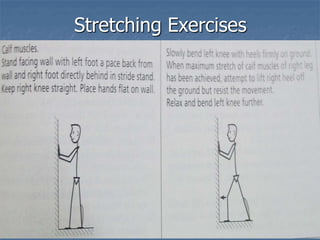



Ankylosing spondylitis is a chronic inflammatory disease that causes stiffness and fusion of the spine. It typically begins in adolescence or early adulthood. Physiotherapy plays an important role in managing ankylosing spondylitis through exercises to improve mobility and flexibility of the spine, strengthen muscles, relieve pain and stiffness, and prevent further fusion of the bones. Treatment includes individual therapies like hydrotherapy, aerobic exercises and stretches, as well as group activities for additional support and education. Regular physiotherapy can help mould fibrous tissue, prevent restricted movement, and maintain physical function for those with ankylosing spondylitis.
























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















