Downloaded 217 times

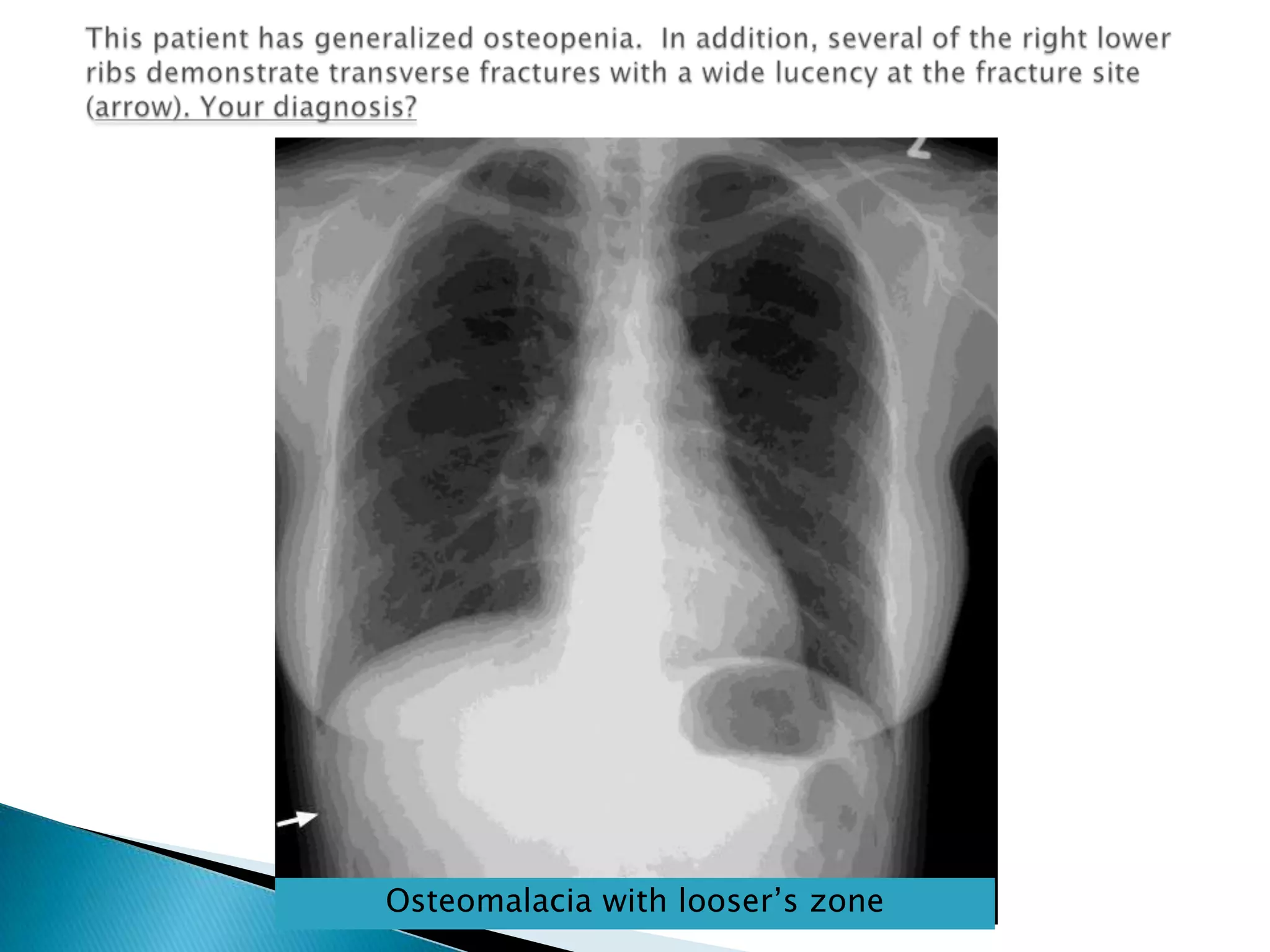
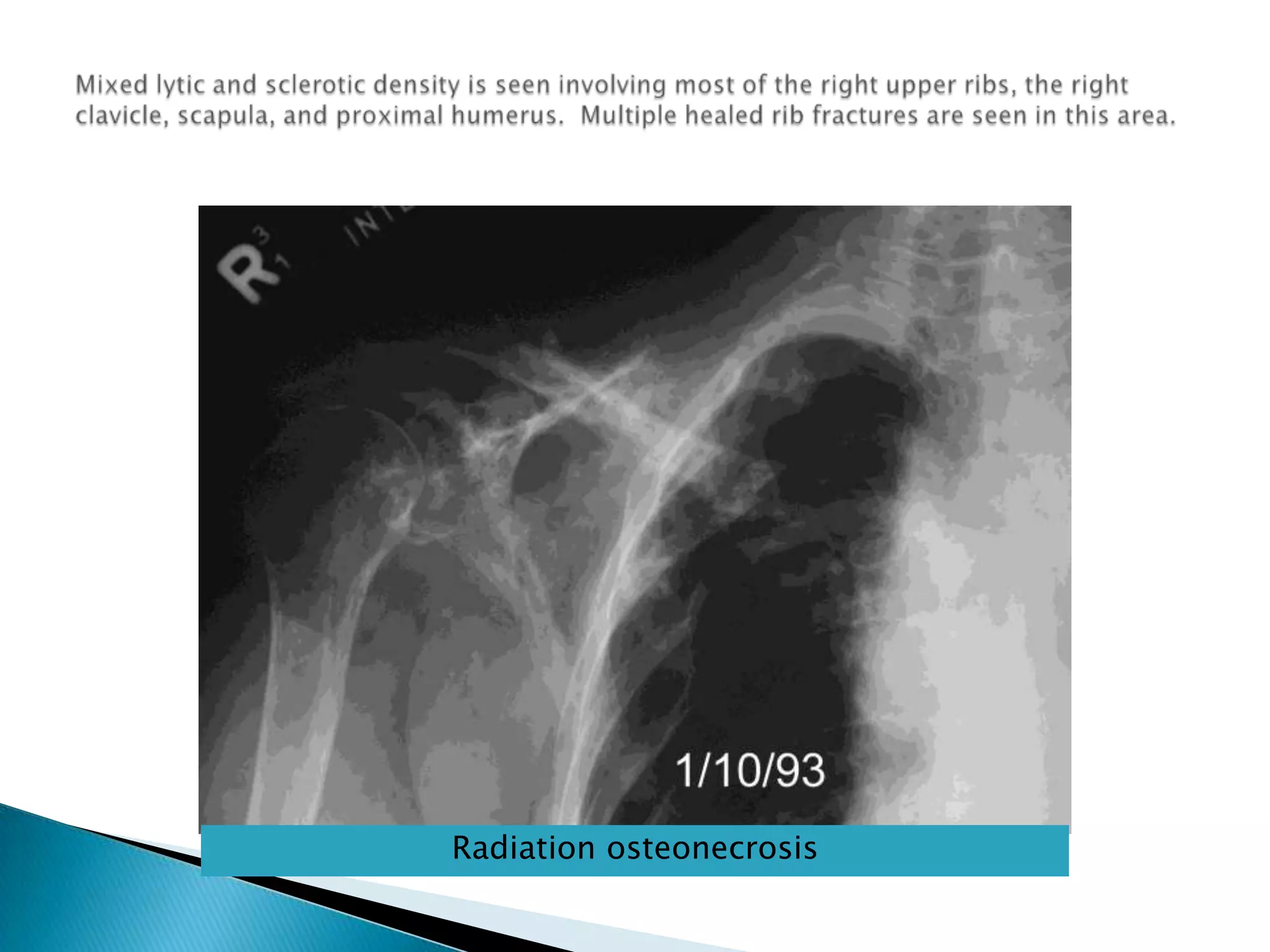


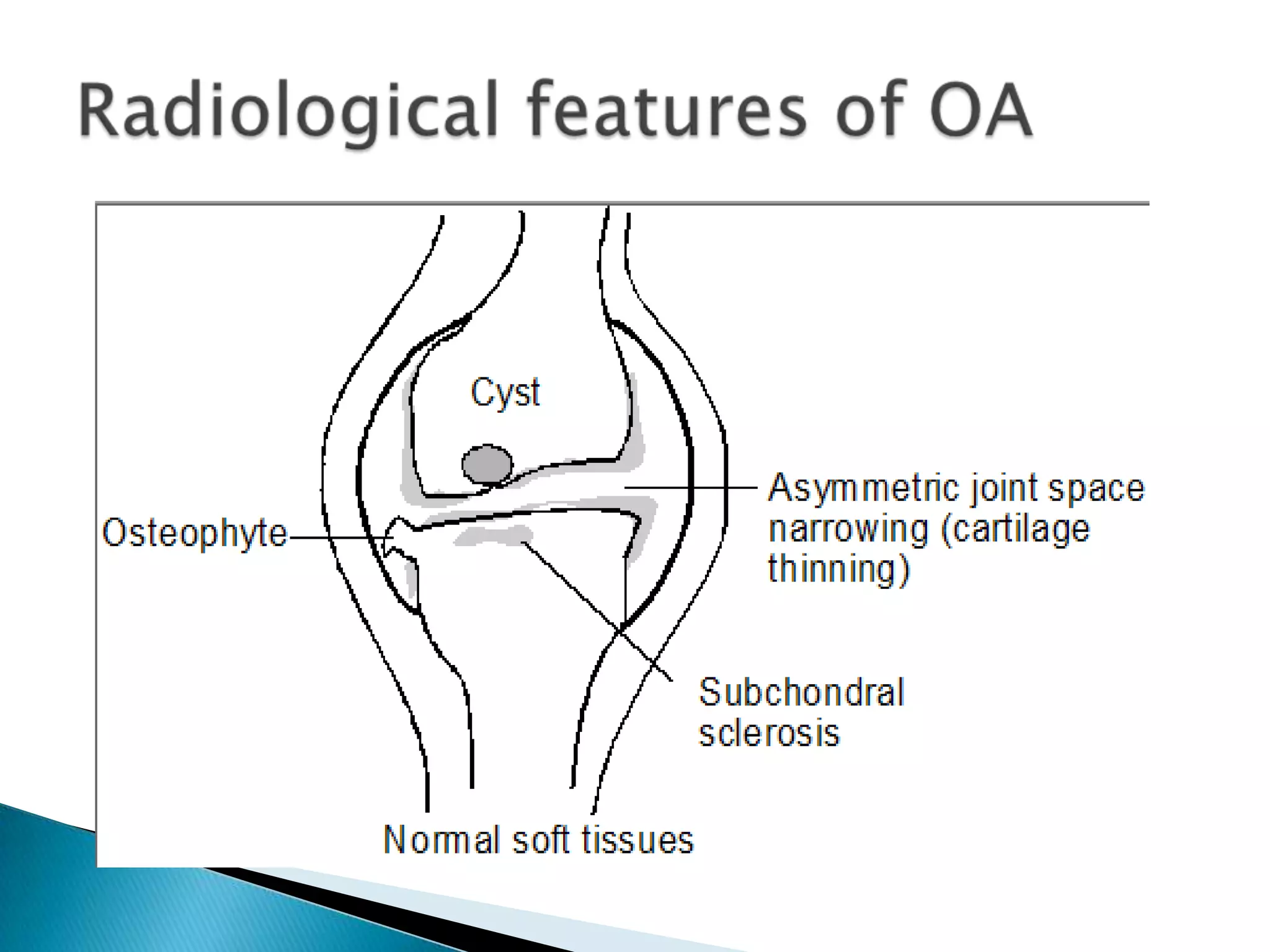
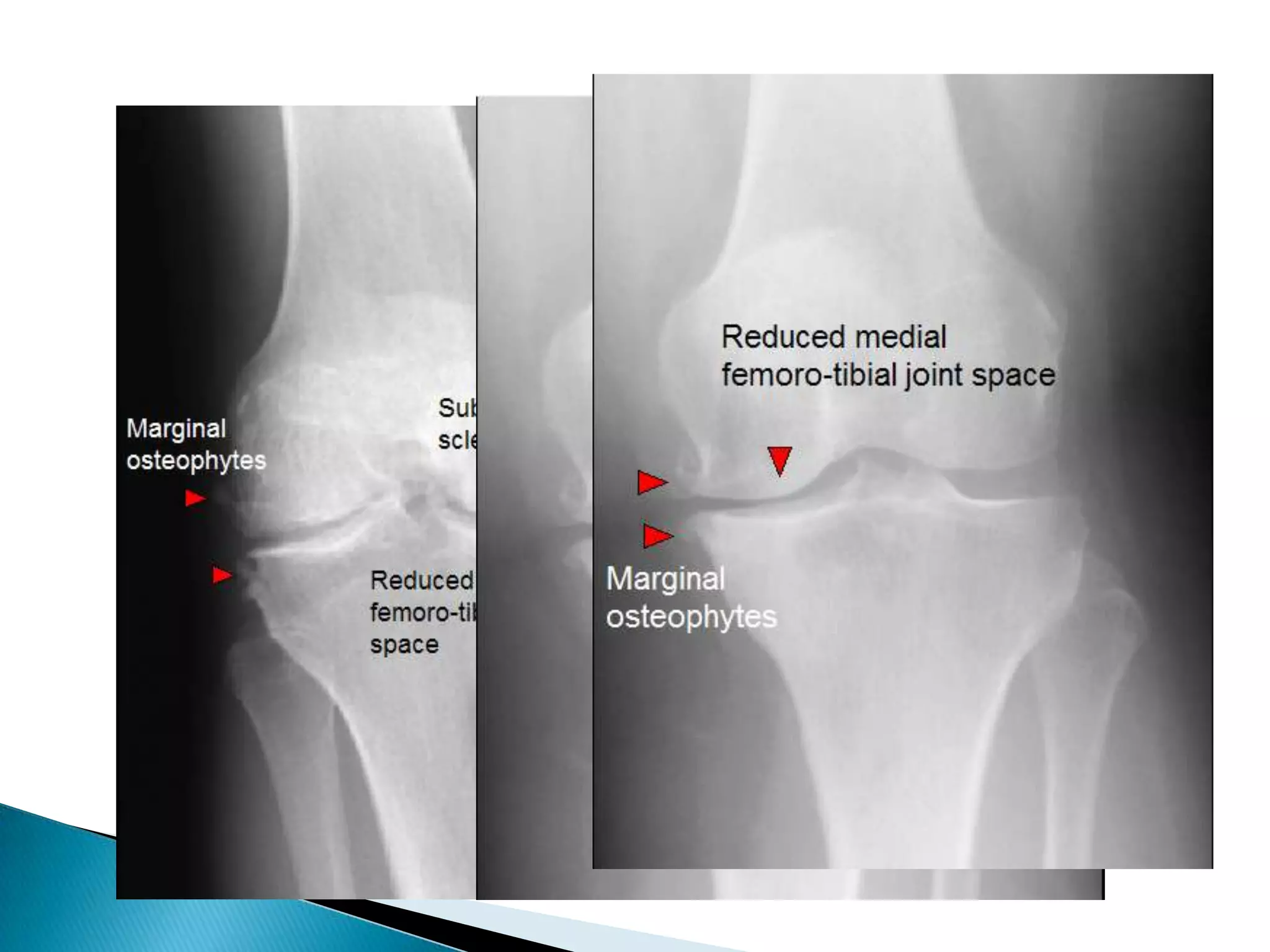
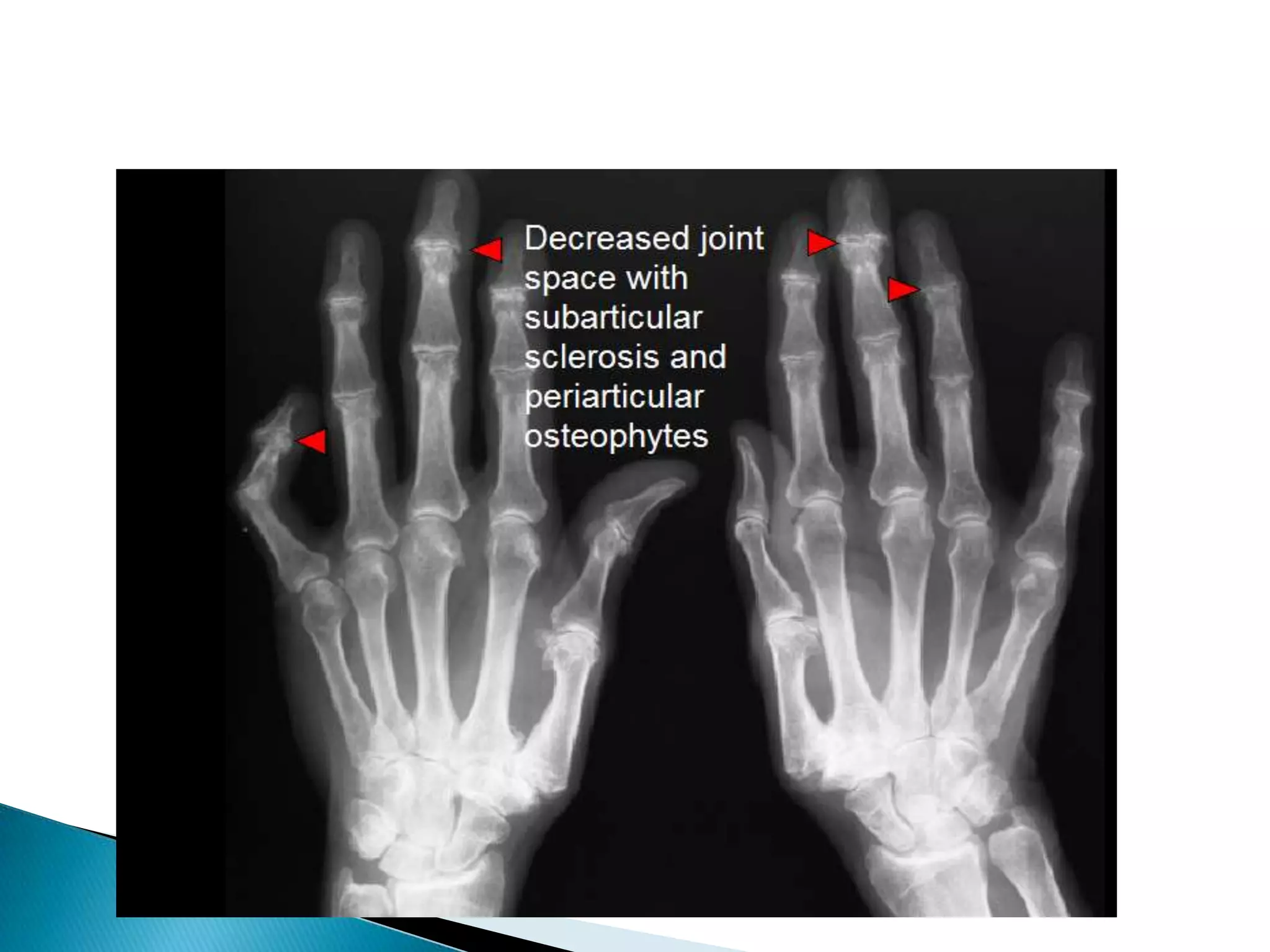

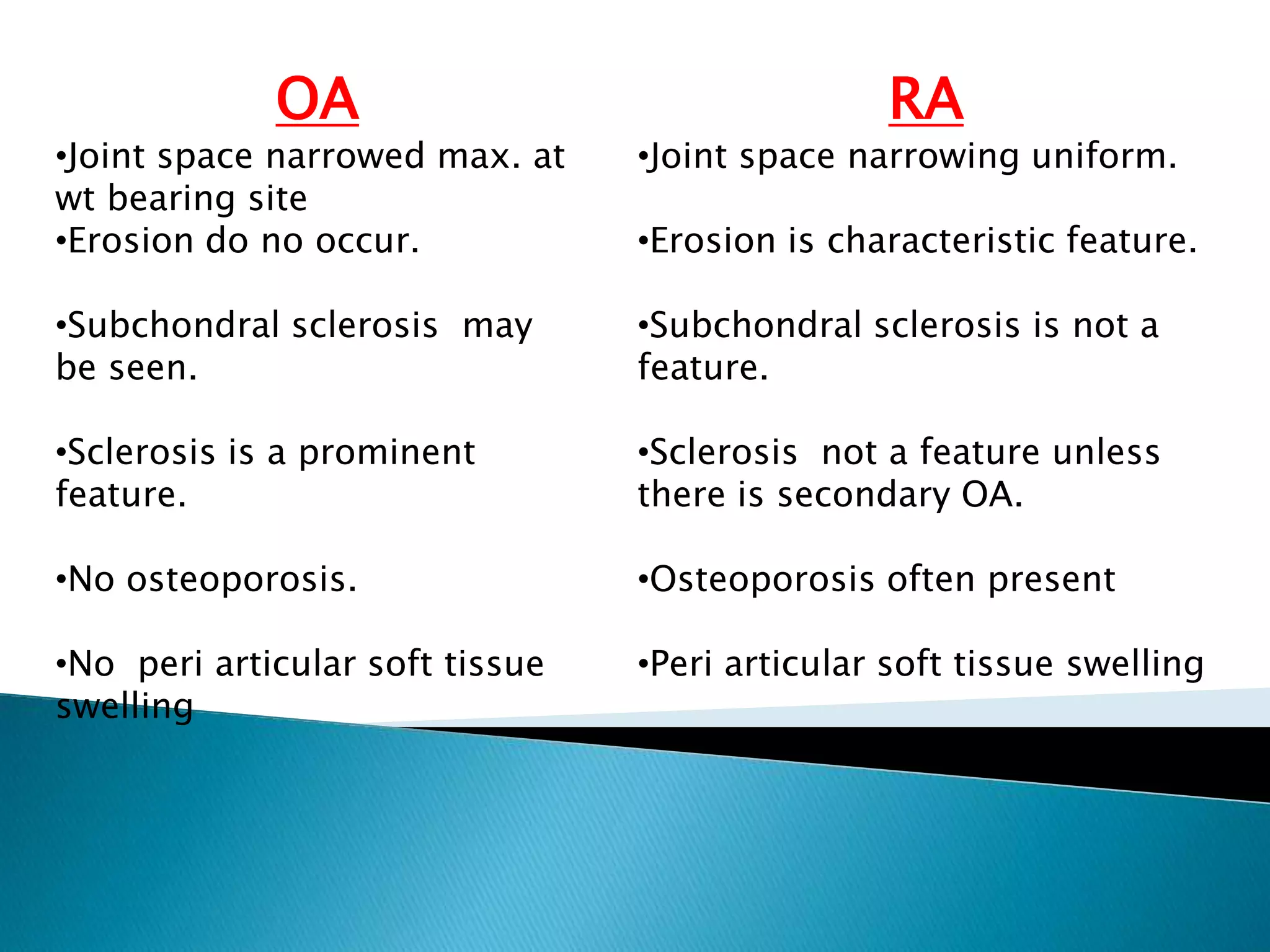
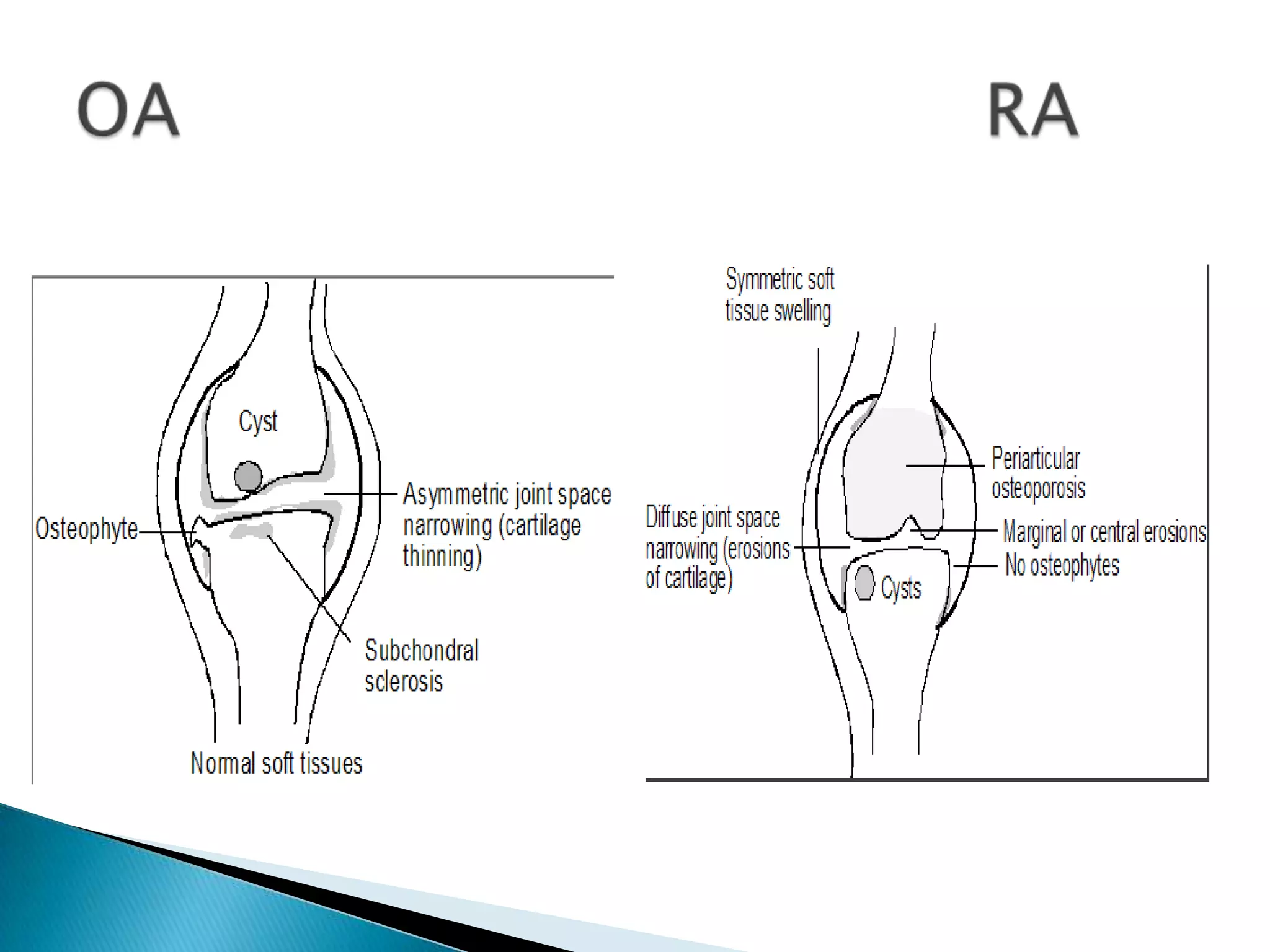



This document discusses various bone and joint diseases and their radiological features. It covers rickets and osteomalacia, noting their effects on bone mineralization and growth plates. Hyperparathyroidism is discussed as causing decreased bone density and subperiosteal bone resorption. Paget's disease causes thickening of bone trabeculae and cortex, leading to bone enlargement. Hemolytic anemias like thalassemia can cause bone marrow hyperplasia seen as thinning cortices and prominent trabeculae. Radiation exposure may lead to osteonecrosis, osteoporosis or sarcomatous changes. Osteoarthritis is characterized by joint space narrowing and subchondral









































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

