This document provides an overview of clubfoot (congenital talipes equinovarus), including:
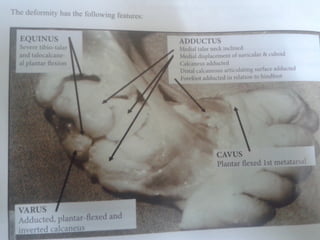
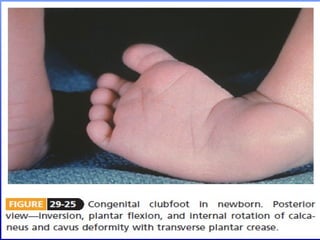
1. The definition, incidence, causes, and typical deformities seen in clubfoot.
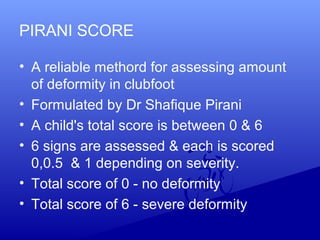
2. Evaluation methods like the Pirani scoring system and radiographic assessment.
3. Treatment approaches like the Ponseti method of serial casting and bracing, as well as surgical options like the McKay procedure when non-operative treatment fails.
4. Post-operative casting protocols and complications that can arise from treatment.


















































![Club foot[1]](https://cdn.slidesharecdn.com/ss_thumbnails/clubfoot1-160908070000-thumbnail.jpg?width=640&height=640&fit=bounds)