Ankylosing Spondylitis
•Download as PPTX, PDF•
46 likes•9,659 views

Ankylosing Spondylitis

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (14)
Similar to Ankylosing Spondylitis
Similar to Ankylosing Spondylitis (20)
More from Gayatri R. Kachh
More from Gayatri R. Kachh (6)
Recently uploaded
Recently uploaded (20)
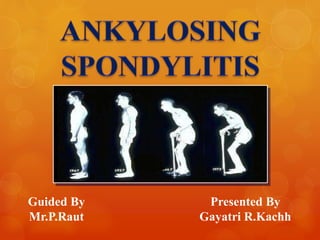
Ankylosing Spondylitis
- 1. Guided By Mr.P.Raut Presented By Gayatri R.Kachh
- 2. Introduction of A.S. Epidemiology of A.S Characteristics Pathological Features of A.S. Symptoms of A.S. Structural Damage in A.S. Causes of A.S. HLA-B27 Pathogenesis of HLA-B27 Diagnosis of A.S. Treatment of A.S. Humira Pen Therapy(Adalimumab) for A.S. Quality of Life Conclusion References
- 3. Ankylosing Spondylitis is a Rheumatic disease of unknown cause that primarily affects the back bone or spine. The name is derived from the Greek words ‘Ankylos” meaning fusion and “Spondylos” meaning vertebra. “Itis” denotes inflammation of the body part. The name therefore describes the inflammatory process in the spinal joints It is considered to be one of a group of diseases called the Spondylo-Arthropathies AS is a chronic, progressive immune-mediated inflammatory disorder that results in ankylosis of the vertebral column and sacroiliac joints Also referred to as the Bekhterev-Strumpell syndrome after the first doctor to actually study the disease. Aka Strumpell-Marie(or Marie- Strumpell) disease after his wife, the first officially noted case study
- 4. First documented AS case was reported in 1691 Unknown cause First signs of Ankylosing Spondylitis were unearthed in the skeletal remains of a 5000 year old Egyptian mummy The incidence of AS may be underestimated due to unreported cases HLA-B27 gene is associated with AS Age of onset typically between 15 and 35 years 2-3 times more frequent in men than in women More common in whites than in nonwhites
- 5. Chronic inflammation in: • Axial structures (sacroiliac joint, spine, anterior chest wall, shoulder and hip) • Possibly large peripheral joints, mainly at the lower limbs (oligoarthritis) • Entheses (enthesitis) Bone formation particularly in the axial joints Serronegative Presence of HLA-B27
- 6. Axial manifestations: Chronic low back pain With or without buttock pain Inflammatory characteristics: Occurs at night (second part), Sleep disturbance,Morning stiffness Limited lumbar motion Onset before age of 40 years Other common symptoms seen during the early stages of disease include: Anorexia Malaise Low grade fever Weight loss Fatigue
- 7. Most striking feature of AS = New bone formation in the spine with: • Spinal syndesmophytes • Ankylosis Both can be seen on conventional radiography Bamboo Spine: Repeated process of healing and bone formation leads to the formation of Syndesmophytes i.e. “Bone Bridges”
- 8. The exact cause of ankylosing spondylitis is unknown, but genes are thought to play a part. The tendency for developing ankylosing spondylitis is believed to be genetically inherited, and the majority (nearly 90%) of patients with ankylosing spondylitis is born with the HLA- B27 gene. The HLA-B27 gene appears only to increase the tendency of developing ankylosing spondylitis One can likely to get AS if you have a history of it in your family. Studies show that almost nine out of ten people with AS have the gene called HLA-B27. Researchers currently think that exposure to certain environmental triggers can lead to the development of AS in people with the gene. But these triggers are unknown.
- 9. Human leukocyte antigens (HLAs) are proteins that help the body's immune system tell the difference between its own cells and foreign, harmful substances. The human leukocyte antigen (HLA) is not a single antigen, but is rather a group of proteins that are located on the surface of White Blood Cells (WBCs). The HLA is the human version of a complex that is known as the major histocompatibility complex. A variation of the HLA-B gene called HLA-B27 increases the risk of developing ankylosing spondylitis. Mechanism of HLA-B27 action in AS patients may still involve peptide handling (the canonical function of HLA- B27 as a MHC class I molecule).
- 10. HLA-B27 is the strongest associated gene in AS. Recent Genome Wide Association Studies (GWAS) have implicated several other genes associated with AS thus affirming the complex, oligogenic nature of the disease HLA-B27 consists of a heavy chain having three a domains, which non-covalently binds short peptides and β2-microglobulin (β2M) Although the HLA-B27 has remained a center of extensive research, the mechanism whereby HLA-B27 confers susceptibility to AS is not well defined. Current hypotheses regarding the pathogenesis of AS have sought to incorporate HLA B27 into mechanistic models.
- 11. MRI X-Ray CT-Scan Several Lab test are also performed such as measuring the concentration of CRP and ESR in the blood samples of A.S. Patients. There is no direct test to diagnose AS
- 12. There is not yet a cure for AS. However, there are effective treatment options that can relieve pain and improve your condition The general approach is a conservative treatment plan that includes: medication, physical therapy, and exercise Drugs like. Local steroid injection To single inflamed joints, entheses, bursae Beware of weight bearing enthesis Not more than 3 injections a yr NSAIDs Spinal stiffness, pain Persistent synovitis or enthesopathy Caution in elderly, peptic ulcer COX II inhibitors Oral or systemic steroids Short courses for intolerable symptoms Uveitis May result in osteoporosis Precipitate heart failure DMARDS & TNF Blocker(Anti-TNF) These are some most frequently used drugs in A.S. Condition
- 13. Right Posture, Swimming, Daily workouts are some of the physical therapies. In severe cases of AS, surgery can be an option in the form of joint replacements, particularly in the knees and hips Daily Workouts Surgery
- 14. HUMIRA (adalimumab) is a recombinant human IgG1 monoclonal antibody specific for human tumor necrosis factor (TNF). HUMIRA is a medicine called a Tumor Necrosis Factor (TNF) blocker. Adalimumab is produced by recombinant DNA technology in a mammalian cell expression system and is purified by a process that includes specific viral inactivation and removal steps. It consists of 1330 amino acids and has a molecular weight of approximately 148 kilodaltons. Adalimumab binds specifically to TNF- alpha and blocks its interaction with the p55 and p75 cell surface TNF receptors.
- 15. AS=23.7 years 90.2 83.1 62.4 54.1 0 20 40 60 80 100 Stiffness Pain Fatigue Poor SleepN=175 PercentageofPatients(%) Bad Quality Pain Sleep problems Fatigue Loss of mobility and dependency Loss of social life Effect employability Higher rate of mortality
- 16. Ankylosing spondylitis has been a challenging disorder with few therapeutic options. In previous studies, patients receiving traditional therapies such as NSAIDs and DMARDs have received only mild to moderate benefit. Importantly, no intervention has been shown to alter progressive loss of spinal mobility. The need for new alternatives for treating these patients is substantial. The pathogenesis of AS is poorly understood. HLA-B27 stands as the earliest and most robust genetic marker associated with a rheumatic disease Researchers are currently exploring the pathogenic role of inflammatory cellular infiltrates, including various cytokines such as TNFα Use TNF inhibitor like Adalimumab(Humira). However, these treatments are of limited benefit. Emerging biological therapies target the inflammatory processes underlying AS, and thus, may favourably alter the disease process while providing relief of symptoms.
- 17. • Anderson JJ. Baron G, van der Heijde D, Felston DT, Dougados M. Ankylosing spondylitis assessment group preliminary definition of short- term improvement in ankylosing spondylitis. Arthritis Rheum 2001;44:1876–86. • Arnett FC. Seronegative spondylarthropathies. Bull Rheum Dis 1987;37:1–12. • Bang, L. M., & Keating, G. M. (2004). Adalimumab: a review of its use in rheumatoid arthritis. Biodrugs 18, 121−139. • Baraliakos et al. Arthritis Research & Therapy 2013, 15:R67 http://arthritis-research.com/content/15/3/R67 • Baraliakos X, Listing J, Rudwaleit M, Sieper J, et al. (2008). The relationship between inflammation and new bone formation in patients with ankylosing spondylitis. Arthritis Res. Ther. 10: R104. • Barliakos X, Haibel H, Listing J, Sieper J, Braun J. Radiographic progression in ankylosing spondylitis – results after up to 8 years of anti-TNF treatment. Ann Rheum Dis 2011; 70 (Suppl 3): 344. • Bartelds, G. M.,Wijbrandts, C. A., Nurmohamed, M. T., Stapel, S., Lems,W. F., Aarden, L., et al. (2007). Clinical response to adalimumab: the relationship with anti-adalimumab antibodies and serum adalimumab concentrations in rheumatoid arthritis. Ann Rheum Dis 66, 921−926. • Bennett PH, Burch TA. The epidemiological diagnosis of ankylosing spondylitis. In: Bennett PH, Wood PHN, eds. Proceedings of the 3rd international symposium of population studies of the rheumatic diseases. Amsterdam: Excerpta Medica Foundation; 1966:305–13. • Bombardieri, S., Ruiz, A., Fardellone, P., McKenna, P., Unnebrink, F., Oezer, K., et al. (2007). Effectiveness of adalimumab in rheumatoid arthritis in patients with a history of TNF antagonists in clinical practice. Rheumatology 46, 1191−1199. • Brewerton D A. HLA-B27 and the inheritance of susceptibility to rheumatic diseases. Arthritis Rheum 1976; 19: 656-68. • Chou CT. Factors affecting the pathogenesis of ankylosing spondylitis. Chin Med J (Engl) 2001;114:212–13. • Galocha, B., Lopez de Castro, J.A. (2010). Mutational analysis reveals a complex interplay of peptide binding and multiple biological features of HLA-B27. J Biol Chem. 285(50), 39180–39190 • Humira (adalimumab) prescribing information. (2007). Abbott Laboratories, North Chicago, IL. • Indian Journal Of Rheumatology 9(2014) 14-18 • Markatseli TE, Alamanos Y, Saougou I, Voulgari PV, Drosos AA: Survival of TNF-alpha antagonists in rheumatoid arthritis: a long-term study. Clin Exp Rheumatol 2012, 30:31-38. • Rheumatology 2014;53:650_657 doi:10.1093/rheumatology/ket387 Advance Access publication 9 December 2013 • Rudwaleit M, Siegert S, Yin Z, Eick J, Thiel A, Radbruch A, et al. Low T cell production of TNFa and IFNg in ankylosing spondylitis: its relation to HLA-B27 and influence of the TNF-308 gene polymorphism. Ann Rheum Dis 2001;60:36–42. • Singh, J. et.al. 2012 Update of the 2008 American College of Rheumatology Recommendations for the Use of Disease-Modifying Antirheumatic Drugs and Biologic Agents in the Treatment of Rheumatoid Arthritis. Arthritis Care & Research Vol. 64, No. 5, May 2012, pp 625–639. Accessed 6/15/2012 Available at: http://www.rheumatology.org/practice/clinical/guidelines/Singh%20et%20al ACR%20RA%20GL- May%202012%20AC&R.PDF. • Ward MM. Functional disability predicts total costs in patients with ankylosing spondylitis. Arthritis Rheum 2002;46:223–31. • Zhang L, Liu JL, Zhang YJ and Wang H (2011). Association between HLA-B*27 polymorphisms and ankylosing spondylitis in Han populations: a meta-analysis. Clin. Exp. Rheumatol. 29: 285-292