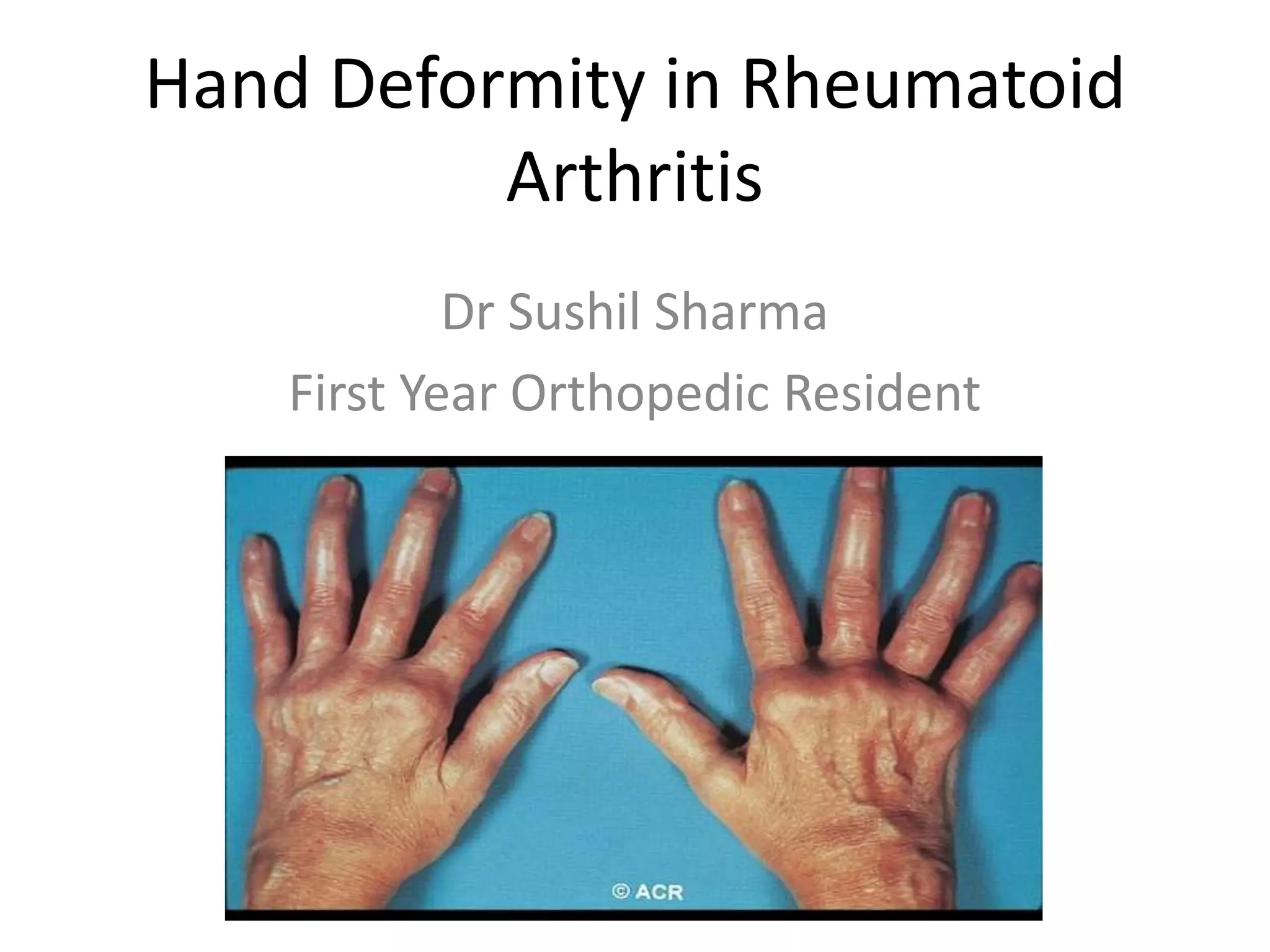
This document discusses hand deformities that can occur in rheumatoid arthritis. It describes how persistent joint inflammation and destruction from RA can lead to articular cartilage erosion, tendon rupture, and capsular stretching, resulting in progressive joint instability and deformities. Common deformities include swan neck, boutonniere, and ulnar deviation of the fingers. The wrist can develop subluxation and collapse. Tenosynovitis is also common in RA and can cause tendon dysfunction and rupture over time. Early treatment is important to prevent permanent hand deformities.