Download as PDF, PPTX
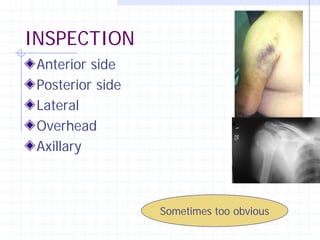
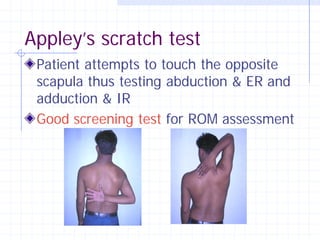


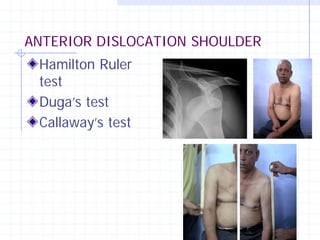
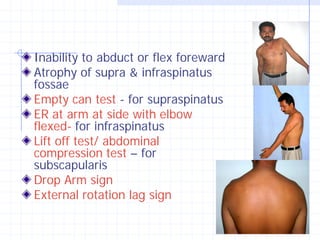
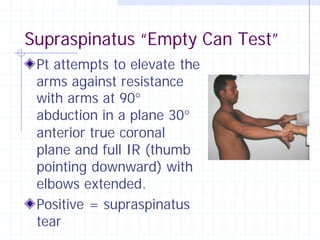
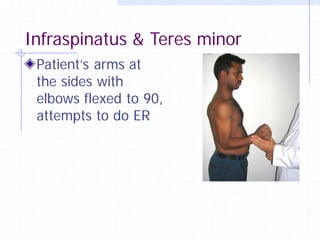



The document outlines the principles and methods for conducting a thorough shoulder examination, including history taking, physical assessment, and specific tests for various conditions such as rotator cuff injuries and instability. It emphasizes the importance of tailored examinations based on patient demographics and presenting symptoms, while highlighting key examinations like Appley’s scratch test and drop arm sign. The document concludes by noting that the clinician's understanding of the patient is critical to effective diagnosis and treatment.





























































































